Korean Rhinoplasty Was Built for Asian Noses. It Now Works on Western Ones Too — Just Not the Same Way.
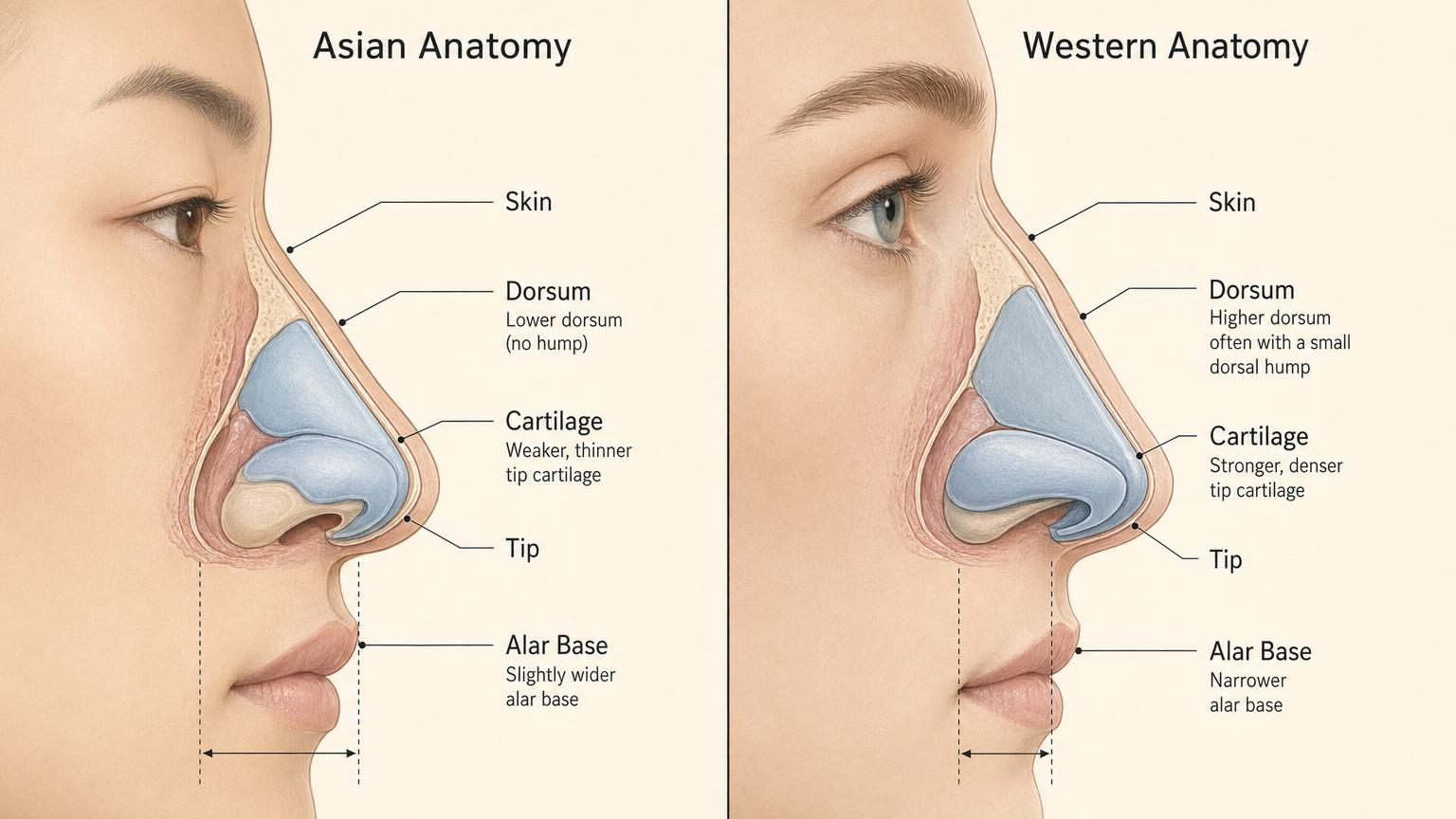
For most of the last twenty years, “Korean rhinoplasty” was a Korean-patient procedure. The technique was developed for the structural realities of an Asian nose — low dorsum, weak tip cartilage, slightly wider base, thicker skin. Western patients flying in for nose surgery typically went to Los Angeles or Istanbul instead, on the assumption that Korean surgeons would not know what to do with a non-Asian nose.
That assumption is no longer accurate. Top Gangnam clinics now see a meaningful percentage of Western patients each year, and the senior surgeons in those clinics have rebuilt their playbook to handle two very different nasal anatomies — Asian and Western — with the same underlying philosophy of restrained refinement. The procedure is genuinely the same. The plan, the cartilage decisions, and the timeline are different.

- Korean rhinoplasty is no longer Asian-only — top Gangnam clinics now run two distinct technical plans depending on whether the patient has an Asian or Western nasal anatomy.
- Asian noses typically need addition (dorsum augmentation with rib or septal cartilage, tip projection, alar narrowing). Western noses typically need subtraction (dorsal hump reduction, tip refinement, sometimes alar base narrowing).
- Both groups get the same Korean restraint philosophy — refinement that preserves identity, not transformation that erases it.
- Recovery is similar in length but differs in detail — Asian patients have slightly more swelling at the tip due to thicker skin envelope, Western patients have slightly more bruising due to dorsal hump work.
- Korean prices: KRW 6M–9M for primary rhinoplasty (USD 4,400–6,700). Comparable U.S. pricing runs USD 8,000–18,000.
- Most Western patients fly home around day 14, not day 7. The dorsal cast comes off at day 7, but residual bruising under the eyes takes longer to fade than tip swelling on Asian patients.
Why the Surgical Plan Looks Different on the Operating Table
Both procedures are called “rhinoplasty.” Both go through the same incisions (open or closed depending on case complexity). Both use the same instruments. The differences are buried in the structural decisions the surgeon makes once the nose is open.
Asian rhinoplasty — additive surgery
For most Asian patients, the goal is to build up. The native dorsum is lower than Western standards consider ideal. The tip cartilage is structurally weaker, so projecting the tip and giving it definition requires reinforcement. The alar base is often slightly wider than the patient wants, which means a small reduction at the nostril sill. The skin envelope is thicker, which is forgiving in some ways (smaller imperfections do not show) but limiting in others (very fine refinements get muffled by overlying tissue).
The Korean surgeon typically uses septal cartilage if available, ear cartilage for tip refinement, and rib cartilage for larger augmentations or revision cases. Implants (silicone or Gore-Tex) are still used widely, though the trend over the last five years has been toward more autologous (your own) cartilage and fewer implants — which is the same direction the rest of the world has moved, just with Korea slightly ahead.
One Korean cafe review at the seven-day mark described the typical experience after combined tip and alar work — “the bruising and swelling settled faster than expected once I followed the post-op care, and the tip is already starting to look defined” — which matches the textbook recovery curve for Asian rhinoplasty patients with thicker skin.
Western rhinoplasty — subtractive surgery
For most Western patients, the goal is to take down. The native dorsum is often higher than the patient wants, sometimes with a visible hump. The tip cartilage is structurally stronger, which means refinement involves trimming and repositioning rather than adding new structural support. The alar base is usually appropriately proportioned, though some patients want subtle narrowing. The skin envelope is thinner, which means the underlying cartilage shape shows through clearly — small irregularities are visible.
The Korean surgeon for a Western patient typically performs a dorsal hump reduction, suture-based tip refinement, sometimes a small alar base narrowing if needed, and almost never adds significant new cartilage. Septal cartilage is still useful for caudal support but in much smaller quantities than in Asian cases.
The thinner skin envelope means the surgical work needs to be cleaner. Any cartilage edge that would be invisible under thicker skin becomes potentially visible under thinner skin. This is the technical difference that makes Western rhinoplasty harder, not easier — despite the procedure being “smaller” in terms of structural change.

The shared philosophy — restraint
Across both groups, what makes the Korean approach distinctive is the philosophy. Korean surgeons design rhinoplasty results that look like a slightly improved version of the patient’s existing nose, not a different nose entirely. The before-and-after compares two photos that obviously belong to the same person. Friends notice that the patient looks better without being able to point to what changed.
This is different from a generic Beverly Hills approach, which tends toward more visible refinement and a more sculpted final shape. It is also different from an Istanbul approach, which has historically optimized for a specific dorsal aesthetic regardless of starting anatomy. Korean restraint is its own school — and Western patients flying to Seoul are increasingly choosing it for that exact reason.
The Korean term for this aesthetic is 자연스러움 (jayeonseureoum) — “naturalness.” It is not just a marketing word. It is a measurable design constraint that runs through every surgical decision.
What Both Plans Cost, and What Recovery Actually Looks Like
This is where the diagnosis turns into a practical comparison. Costs and recovery patterns differ between Asian and Western cases in specific, predictable ways.
| Procedure | Korea (KRW) | USD | U.S. comparable |
|---|---|---|---|
| Primary rhinoplasty (Asian) | 6M – 9M | $4,400 – $6,700 | $8,000 – $14,000 |
| Primary rhinoplasty (Western) | 7M – 10M | $5,200 – $7,400 | $10,000 – $18,000 |
| Revision rhinoplasty | 9M – 14M | $6,700 – $10,400 | $12,000 – $25,000 |
| Alar reduction only | 2M – 3M | $1,500 – $2,200 | $3,500 – $6,000 |
Established Gangnam clinics that publish surgeon-specific galleries — including Link Plastic Surgery’s rhinoplasty page — sit in the middle of these ranges. Cheaper quotes from app-based platforms typically exclude the design consultation, exclude follow-up visits, or assume a junior surgeon rather than the senior one in the photos.
Day 1 — splint, bruising, and tape

Both Asian and Western patients leave the clinic with a small dorsal splint or cast taped across the bridge of the nose. This stays in place for seven days, kept dry. There is also internal nasal packing or stents in some cases, removed at day three to five depending on the surgeon.
The pain is genuinely minimal — patients consistently describe pressure rather than pain, similar to a sinus infection. The medication regimen is short, usually three to five days of antibiotics and a milder analgesic.
Day 7 — cast comes off, bruising is yellow-green

Day seven is the milestone every rhinoplasty patient counts down to. The dorsal cast comes off, the surgeon checks the early shape, and the patient sees the new nose for the first time without the cast covering it. The nose looks swollen — about 30 to 40 percent more swelling than the final shape — but the new bridge profile is already visible.
Bruising under the eyes has shifted from purple-blue to yellow-green by this point. Concealer covers most of it. Sunglasses cover the rest. This is the day Asian patients typically return to office work in Korea. Western international patients usually need a few more days because the under-eye bruising has farther to fade on lighter skin tones.
Day 14 — flying home and the first social re-entry
For Western patients flying internationally, day 14 is the realistic comfortable departure day. Bruising is faded to a faint yellow tinge that concealer hides completely. The nose still looks swollen — particularly at the tip if the patient had tip refinement — but the swelling pattern is no longer obviously surgical from a normal viewing distance.
Asian patients are usually further along at this point because they had less dorsal work and therefore less bruising. The tip swelling is the persistent feature for them, and it takes the longest to resolve.
Month 3 — what the photos look like

By the three-month mark, the dorsum is fully settled. The tip swelling has dropped to about 90 percent resolved — the remaining 10 percent settles over months four through twelve, particularly for thicker-skinned Asian patients. Most Asian patients reach final shape around the one-year mark. Most Western patients reach final shape around month six because there is less residual tip edema to resolve.
The before-and-after comparison at three months looks dramatic on a Western patient (where the dorsal change is visible from any angle) and subtle on an Asian patient (where the change is most visible in three-quarter view but understated in front view). Both outcomes are intentional. Both are what the patient came for.
Frequently Asked Questions
Can I get good rhinoplasty in Korea if I’m not Asian?
Yes, at top Gangnam clinics with surgeons who have specific training in Western nasal anatomy. Not every Korean surgeon does this — many specialize exclusively in Asian rhinoplasty. Look for surgeons whose published gallery includes Western patient cases, or contact the clinic in advance and ask explicitly whether the surgeon you would be assigned has experience with non-Asian noses. Several Gangnam clinics — including Link Plastic Surgery — publish surgeon-specific galleries that show this distinction openly.
Will my nose look “Asian” if I’m Western and have surgery in Korea?
No, if you choose a surgeon trained for Western anatomy. The Korean restraint philosophy applies to your starting structure — the surgeon refines the nose you have, not transforms it into a different aesthetic. The before-and-after looks like the same person with a slightly cleaner profile.
Open vs closed rhinoplasty — does it matter?
For most cases, no — both approaches give comparable results in experienced hands. Closed (incisions inside the nostrils only) leaves no external scar and has slightly less tip swelling. Open (a small incision across the columella) gives the surgeon better visibility and is preferred for revision cases or complex tip work. The columellar scar fades to invisible by month three to six.
How long does the swelling actually last?
The 80 percent of swelling resolves by month one. The 90 percent point is around month three. The final 10 percent — the persistent tip edema that only the patient and the surgeon notice — takes six months on Western patients and twelve months on Asian patients with thicker skin. Plan accordingly if you are choosing a wedding date or major event.
What if I want a revision after a previous rhinoplasty done elsewhere?
Revision rhinoplasty in Korea is a separate specialty from primary. The surgeons who do revision well are a subset of surgeons who do primary well. Korean revision specialists handle cases from all over the world, including patients whose original surgery was done in Istanbul, Los Angeles, or local Korean clinics. The dedicated revision rhinoplasty page at established clinics typically goes into the criteria more deeply than primary rhinoplasty does.
Is rib cartilage really necessary?
For Asian primary rhinoplasty, rib cartilage is one option among several — septal and ear cartilage are more common for first-time cases. Rib becomes the standard choice for revision cases or for very large augmentations where there is not enough donor cartilage available elsewhere. For Western primary rhinoplasty, rib cartilage is rarely needed because the surgery is mostly subtractive.
Will I be able to fly home with the cast on?
Yes, the cast is travel-safe and most patients keep it on through their first flight if they leave Korea between day three and day six. The cabin pressure does not cause issues. By day seven the cast comes off either at the Korean clinic before departure or at home — most surgeons are flexible about which.
How do I find a surgeon trained for both Asian and Western noses?

Look for a board-certified Korean plastic surgeon (성형외과 전문의) with a documented gallery that explicitly includes both Asian and Western patient cases. Avoid clinics that only show Asian results — that does not mean they are bad surgeons, it means they specialize in one anatomy. Senior surgeons at established Gangnam clinics with international patient programs are the safest filter.
Ask the clinic specifically whether the surgeon you would be assigned (not just “the clinic” generally) has handled cases similar to yours. The answer should include specific numbers — how many revision cases, how many Western primaries, what percentage of their practice is each. If the clinic cannot answer that question, walk out.
Recommended for Your Recovery
Products patients commonly use during the rhinoplasty recovery window — same items routinely included in the post-op kits Seoul clinics hand out at discharge.
- Arnica Montana Tablets — start 3 days before surgery to reduce bruising, especially helpful for Western patients with thinner skin who tend to bruise more visibly. Check price on Amazon
- Bromelain Supplement (500mg) — natural anti-inflammatory commonly recommended by Korean clinics for nasal procedures to speed swelling resolution. Check price on Amazon
- Gel Eye Mask (Cold Compress) — reusable cold pack for the under-eye bruising that follows dorsal hump reduction work. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — lightweight Korean sunscreen for the healing nasal skin once the cast is off (week 2 onward) to prevent post-inflammatory pigmentation. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.