Korean Breast Lift (Mastopexy): Why Implants Don’t Fix Sagging, and the Ptosis Grade That Decides Your Surgery
There is a moment that happens in almost every breast consultation with a foreign patient, and it happens before anyone has measured anything. The patient sits down and says some version of the same sentence. My breasts used to sit higher. After two pregnancies, or after losing twenty kilos, they dropped and lost their shape. I want a breast augmentation to fix it.
And the Korean surgeon, listening carefully, already knows that the patient has described the right problem with the wrong solution. What she is describing is a position problem. What she is asking for is a volume operation. Those are not the same surgery, and confusing them is the most expensive mistake in breast aesthetics. If you have spent any time on this site, you may have read our guide to Korean breast augmentation with Mentor implants, and it is excellent for the patient who genuinely needs more volume. This article is about the patient who does not, and who often gets an implant anyway and ends up unhappier than before. We will walk through how a Korean surgeon grades sagging, why an implant alone usually makes a sagging breast worse, and which operation each grade actually needs. If you want to discuss your own case, you can book a consultation at Link Plastic Surgery and have your ptosis graded properly before anyone talks about implants.

The Most Common Breast Surgery Mistake Foreign Patients Make
Walk into a Gangnam consultation room with a printout of an implant size you found online, and a good surgeon will gently set it aside. Not because implants are wrong, but because the size of the implant is the last thing that should be decided, not the first. Before any number gets discussed, the surgeon needs to answer one question. Is this a volume problem or a position problem?
Here is the difference in plain language. A volume problem is when you have lost fullness, usually in the upper part of the breast, and the tissue that remains still sits where it should. The breast looks deflated but not droopy. A position problem is when the whole structure has migrated downward. The nipple sits lower than it used to. The tissue hangs below the natural crease underneath the breast. There may be loose, stretched skin that no bra fully disguises. This downward migration has a clinical name, ptosis, and it is what most patients are actually describing when they say their breasts lost their shape after pregnancy or weight loss.
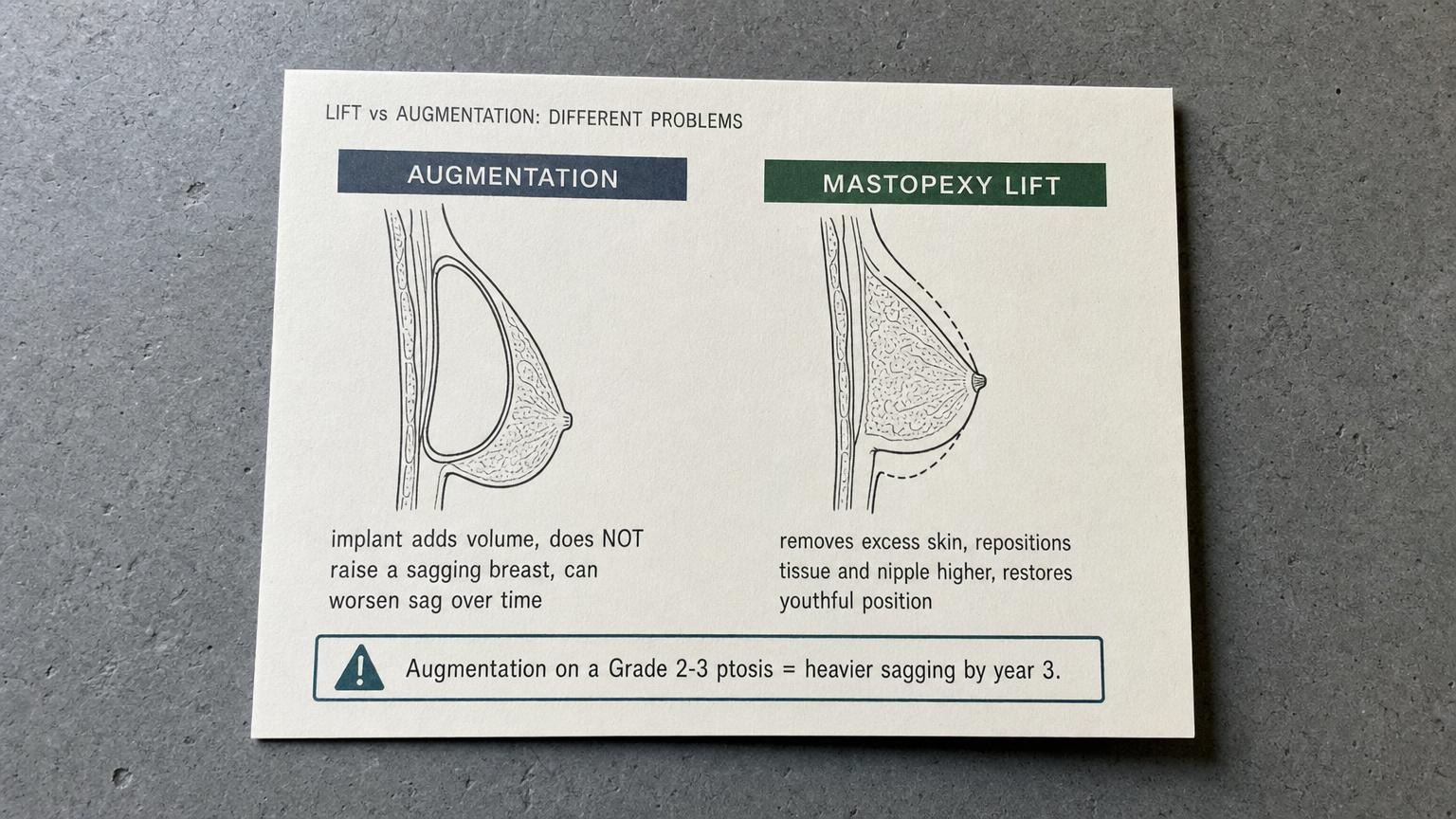
Now here is why the distinction is not academic. Imagine a breast that has already stretched and dropped, with a skin envelope that has lost its tone. An implant is a weight. Placing a weight inside an envelope that has already failed to hold the tissue up does not pull anything higher. It adds load to a structure that is already losing the fight against gravity. The implant fills out the lower pole, the nipple still points down, and within a year or two the breast sags further, now heavier and lower than before surgery. Surgeons call the late version of this bottoming-out, and revision clinics in Seoul see a steady stream of patients who arrived with sagging, got an implant, and came back worse. The implant did exactly what implants do. It added volume. It was simply asked to do a job it cannot do.
This is why the Korean approach reverses the usual order. The surgeon assesses ptosis grade first, on the examination table, with measurements, and only then has a conversation about whether you need a lift, an implant, or both. The complaint that brings most post-pregnancy and post-weight-loss patients into the room is a lift complaint. The honest answer is rarely the one they walked in asking for, and a surgeon who agrees too quickly to a simple augmentation is often the one to be careful of.
Ptosis Grades: The Measurement That Determines Everything (Regnault Classification)
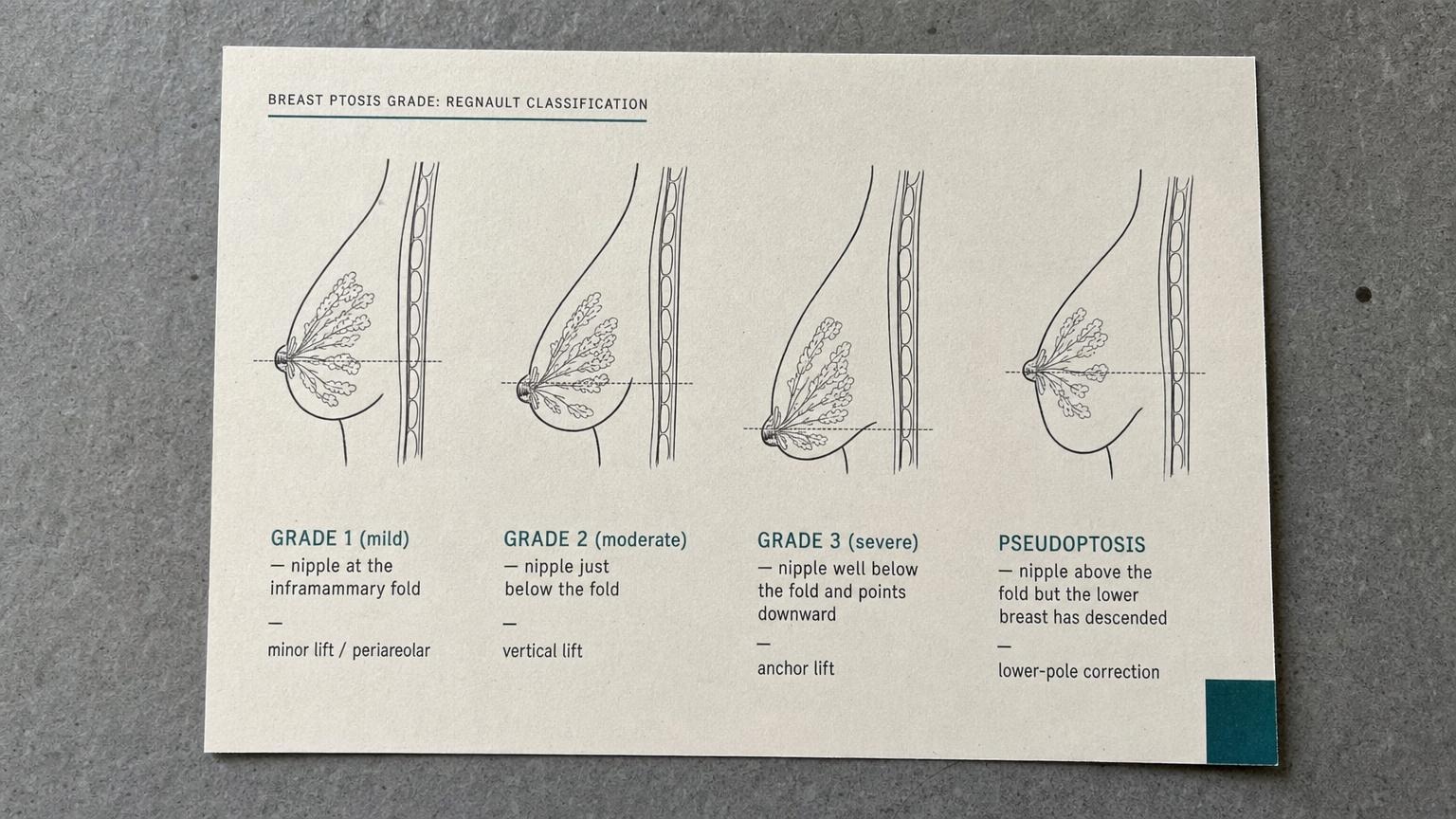
The reason Korean surgeons can be precise rather than vague about your options is that breast sagging is measured, not eyeballed. The standard tool is the Regnault classification, and the single landmark that everything turns on is the inframammary fold, the natural crease where the bottom of the breast meets the chest wall. The position of the nipple relative to that fold tells the surgeon almost everything about which operation you need.
Grade 1, mild ptosis, means the nipple sits right at the level of the fold. The breast has dropped a little, but the nipple still sits at or just above the crease and points forward. This is the most forgiving grade, and it is the one most likely to be improved with a minimal lift or, in the right patient, with volume alone.
Grade 2, moderate ptosis, means the nipple has dropped below the fold but still points forward rather than down. This is the bracket that a large share of post-pregnancy patients fall into, and it is also the bracket where the implant-only mistake does the most damage. A Grade 2 breast genuinely needs the nipple and tissue raised. An implant placed without a lift here is the classic recipe for the breast that looks worse by year three.
Grade 3, severe ptosis, means the nipple has dropped well below the fold and now points downward toward the floor. The tissue hangs, the skin envelope is significantly stretched, and the only honest path to a youthful shape is a substantial lift, often with the most complete incision pattern. No implant on its own will rescue a Grade 3 breast, and any clinic that suggests otherwise is selling, not diagnosing.
There is one more category that sits outside the simple ladder, and it matters enormously for the volume-versus-lift decision. It is called pseudoptosis, false sagging. In pseudoptosis the nipple is still in a good position, at or above the fold, but the gland itself has emptied and slumped below it, usually after breastfeeding. The breast looks droopy in a bra, but the actual problem is lost volume in a relatively well-positioned envelope. Pseudoptosis is the one presentation where an implant alone, or an implant with only a minor skin adjustment, can be the correct answer, because the position of the nipple does not need to change. Telling true Grade 2 ptosis apart from pseudoptosis is one of the most important judgments your surgeon makes, and it is invisible to a patient looking in the mirror. It requires hands-on measurement. This is the entire reason the grading has to come before the implant talk.
Lift vs Augmentation vs Both: How Korea Decides
Once your ptosis grade and skin quality are on the table, the surgery splits into three honest paths. Each one solves a different problem, and the Korean philosophy is to match the operation to the anatomy rather than to the patient’s opening request.
Recommended for Your Recovery
Products commonly used before and after Korean breast lift mastopexy vs augmentation — same items routinely recommended in the recovery instructions Seoul clinics hand out at discharge.
- Arnica Montana Tablets — start 3 days before body surgery to reduce bruising in the treated zone. Check price on Amazon
- Silicone Scar Sheets — cut to size and apply over incision lines starting week 3 to flatten scar formation. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — daily UV protection on healing scars — sun exposure during the first 6 months drives post-inflammatory pigmentation. Check price on Amazon
- COSRX Advanced Snail 96 Mucin Power Essence — gentle Korean skin essence to support overall skin barrier during the recovery window. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
Pure augmentation. This is an implant alone, with no skin removal and no nipple repositioning. It is the right choice for a narrow group, mainly pseudoptosis and genuine volume loss where the skin still has tone and the nipple still sits in a good position. If your real complaint is emptiness rather than droop, and your surgeon confirms the envelope has not stretched, then volume is the clean answer and you can read our full account of the implant choice and recovery in the Korean breast augmentation guide. The augmentation-only approach is the wrong answer the moment skin laxity enters the picture.
Pure mastopexy, the lift. This is the operation that actually addresses sagging. The surgeon removes the excess, stretched skin, lifts the breast tissue, and repositions the nipple and areola higher on the chest so they point forward again. No implant is placed. It is the right choice when you have enough of your own volume but the structure has dropped, which describes a great many Grade 2 and some Grade 3 patients who are happy with their size and only want their shape back. A lift will not make you bigger. It makes what you have sit where it used to.
Augmentation plus lift, the combined procedure. This is for the patient who wants both, a higher position and more fullness, particularly in the upper pole that deflates after breastfeeding. It is the most technically demanding of the three because the surgeon is doing two opposing things at once. The lift tightens and reduces the skin envelope, while the implant expands it, and those forces work against each other. Korean surgeons handle this carefully, performing it in a single well-planned session for moderate cases and staging it across two surgeries when the ptosis is severe or the tissue is very thin and the risk of wound tension is high. If a clinic offers you a combined lift and large implant casually, as if it were no harder than a simple augmentation, that is a warning sign.
The rule that ties all three together is the one nobody selling you an implant wants to say out loud. Putting an implant into a Grade 2 or Grade 3 breast without a lift does not fix the sag. It buries the problem under volume for a few months and then hands it back to you heavier. The breast settles around the implant, the nipple stays low, and the result drifts toward the very revision case that fills Seoul’s correction clinics. You can see the broader landscape of body procedures and how they combine on the Link Plastic Surgery body surgery hub. The point is simple. Grade first, then choose. Never the other way around.
Incision Patterns and the Scar Tradeoff
If you decide on a lift, the next honest conversation is about scars, because a lift trades a scar for a position. There is no scarless mastopexy for moderate or severe sagging, and any promise of one is a red flag. What a good surgeon offers instead is the smallest incision pattern that will hold the result, matched to how much skin has to come out. There are three patterns, and they scale with your ptosis grade.
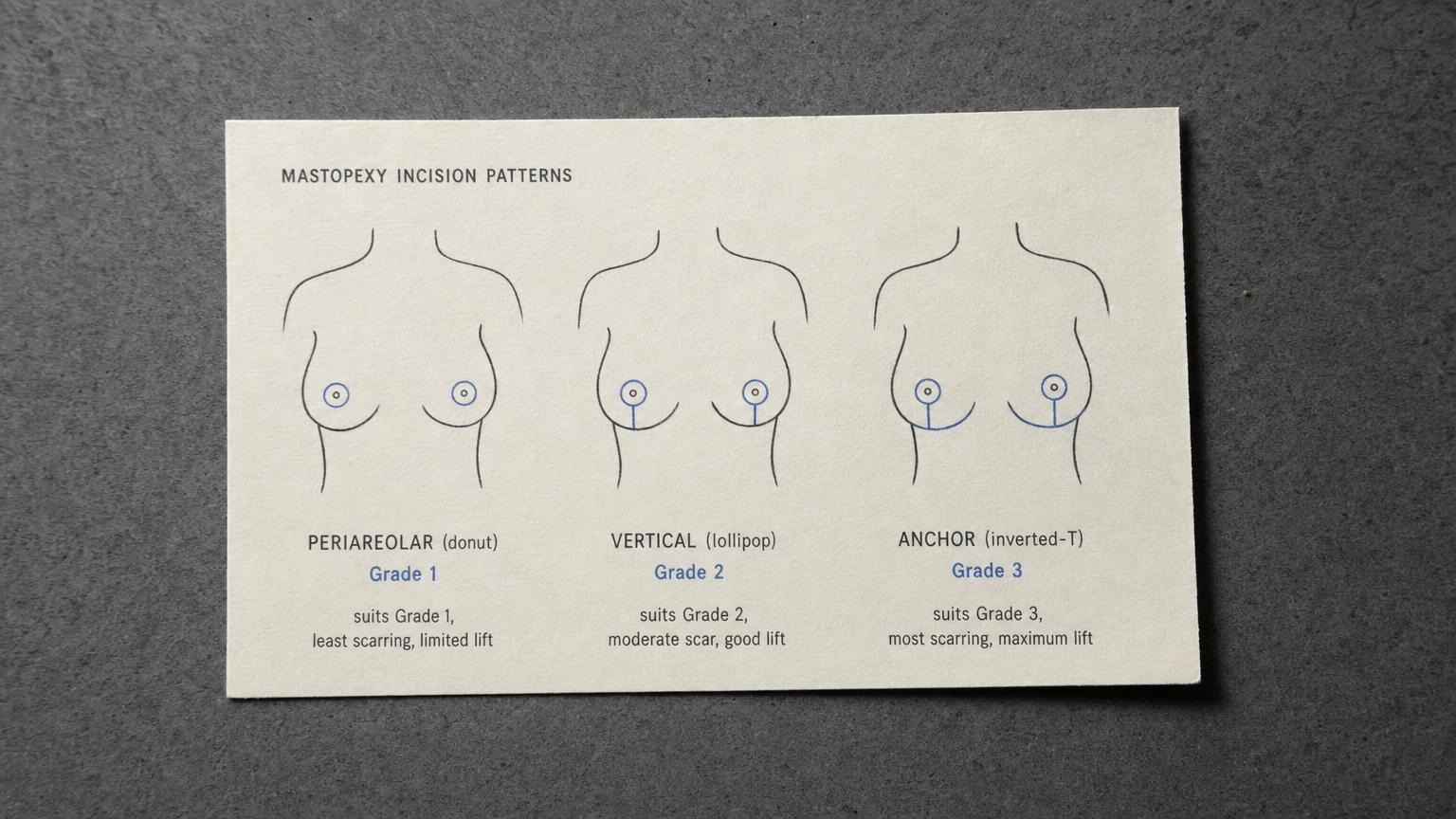
The periareolar pattern, often called the donut, places the incision around the border of the areola where the colored skin meets the lighter skin. It is the most discreet because the scar hides at a natural color transition. It only suits mild ptosis and small lifts, because the amount of skin it can remove is limited. Push it beyond its range and you risk a flattened breast and a widened areola, so a careful surgeon will not use it for a Grade 2 or Grade 3 breast.
The vertical pattern, the lollipop, adds a single vertical line running from the bottom of the areola down to the inframammary fold. It removes more skin and gives a stronger, more reliable lift, and it is the workhorse of Korean mastopexy for moderate ptosis. The vertical scar is genuinely there, but it sits on the front of the breast in a line that fades well and is hidden by almost any clothing. For most Grade 2 patients, this is the pattern that balances lift and scar best.
The anchor pattern, the inverted-T, adds a horizontal scar running along the inframammary fold on top of the vertical and periareolar incisions. It removes the most skin and gives the most powerful lift, which is why it is reserved for severe Grade 3 ptosis and large, heavy breasts that the smaller patterns cannot stabilize. The horizontal limb hides in the crease underneath the breast, but the overall scar footprint is the largest of the three. The tradeoff is honest. More scar buys more lift and more durability.
The Korean approach favors the least scar that achieves a stable lift, never the least scar that looks good on day one and fails by year two. Beyond pattern choice, the difference between a fine pale line and an obvious scar usually comes down to closure technique and aftercare, meticulous layered suturing that takes tension off the skin, plus a scar protocol of silicone, sun protection, and sometimes laser starting at around week six. Done well, even an anchor scar matures into a quiet, pale line over 6 to 12 months. What you should never accept is a surgeon who is vague about scars. A good one will draw the exact pattern on you and tell you precisely where the lines will sit.

Cost, Recovery, and What Korean Mastopexy Includes
Price for a lift depends heavily on your grade, your incision pattern, and whether an implant is added, but here is a realistic frame for international patients comparing Seoul against home.
| Procedure | Korea (Seoul) | USA | Australia |
|---|---|---|---|
| Breast lift (mastopexy) alone | KRW 6,000,000 to 10,000,000 (approx USD 4,400 to 7,300) | USD 9,000 to 15,000 | AUD 14,000 to 22,000 |
| Lift plus augmentation (combined) | KRW 9,000,000 to 14,000,000 (approx USD 6,600 to 10,200) | USD 13,000 to 20,000 | AUD 20,000 to 30,000 |
| Revision after bottomed-out implant | Quoted per case after exam | USD 12,000 to 22,000 | AUD 18,000 to 32,000 |
| Scar management package | Usually included in Korean fee | Often billed separately | Often billed separately |
What the Korean fee typically folds in, where Western quotes often do not, is the follow-up. Suture checks, early wound review, the scar protocol, and remote photo follow-up after you fly home are generally part of the package rather than line items. That bundling is part of why the headline numbers look lower.
Recovery follows a predictable arc. A surgical support bra is worn for around six weeks to hold the new shape while the internal tissues settle. Desk work is realistic at two to three weeks, with no lifting or overhead reaching during that window. Scar management begins around week six, once the incisions have fully sealed, and continues for months. Swelling resolves over six to eight weeks, and the final shape along with full scar maturation takes 6 to 12 months. Many patients pair a lift with other body work in a single trip, and if you are considering a fuller reshaping, our guides to Korean liposuction and body contouring and to the postpartum combination in our Korean tummy tuck and mommy makeover coverage explain how surgeons stage these safely together.
Before you book, take five questions into the consultation and judge the surgeon by the answers. First, did the surgeon actually grade your ptosis on the exam table, or just look at a photo? Second, do you need a lift, an augmentation, or both, and what is the reason for that recommendation in your specific anatomy? Third, which incision pattern will be used, and exactly where will the scars sit? Fourth, what is the year-five outlook for your tissue, given your skin quality and any plans for pregnancy? Fifth, who handles your remote follow-up and a possible revision once you have flown home? A surgeon who answers all five clearly is treating your case. A surgeon who jumps straight to implant brands and sizes is selling you a volume operation you may not need.

Frequently Asked Questions
Will a breast implant lift my sagging breasts?
No. An implant adds volume and fills the upper pole, but it does not raise a low nipple or remove loose skin. On a Grade 2 or Grade 3 ptosis, an implant adds weight to an already lax envelope, so the breast tends to sag further around the implant within a couple of years. Real lifting comes from a mastopexy, which removes excess skin and repositions the nipple and tissue higher. If you want both a higher position and more volume, you need a lift, with or without an implant added.
Can I get a lift to fix a botched augmentation that now sags?
Often yes. A common revision is bottoming-out or sagging after an implant was placed into ptosis that was never lifted. The correction usually combines a mastopexy with implant assessment, sometimes downsizing or repositioning the implant and tightening the lower pole. A Korean surgeon will re-grade your ptosis, check the implant pocket, and decide whether a lift alone, a lift plus implant exchange, or implant removal with lift is the cleaner result for your tissue.
Will I lose volume if I only get a lift without an implant?
A pure lift reshapes and repositions the tissue you already have. It does not add volume, and the upper pole can look a little less full than an implant would make it, especially if you started with deflated tissue after pregnancy or weight loss. If you have enough volume and only dislike the position, a lift alone is ideal. If you also want more fullness, the plan becomes a lift plus a small implant or, in some cases, fat grafting to the upper pole.
Is a combined lift plus implant safe in one session?
It can be, but it is technically demanding because the surgeon is tightening the skin envelope and adding volume to it at the same time, and those two forces pull against each other. Many Korean surgeons do it in one carefully planned session for moderate cases, and stage it across two surgeries for severe ptosis or very thin tissue. The decision depends on your ptosis grade, skin quality, and how much volume you want. Ask your surgeon directly whether one stage or two is safer for your specific anatomy.
How visible are mastopexy scars, realistically?
A lift trades a scar for a position, and there is no scarless lift for moderate to severe sagging. A periareolar (donut) scar hides at the areola border and suits mild lifts. A vertical (lollipop) scar adds a line from the areola to the fold. An anchor scar adds a horizontal line hidden in the inframammary crease for larger lifts. Korean surgeons favor the smallest pattern that gives a stable result and use meticulous closure plus a scar protocol from week six. Most scars mature to a fine pale line over 6 to 12 months.
Can I breastfeed after a breast lift?
Many women can, but it is not guaranteed. Most modern mastopexy techniques keep the nipple attached to its blood supply and milk ducts on a tissue pedicle, which preserves function better than older methods. Even so, any breast surgery can reduce milk supply. If you plan to have children and breastfeed, tell your surgeon before surgery so the technique can be chosen with that in mind, and discuss timing, since many surgeons advise lifting after you have finished having children.
Does Asian breast tissue change the lift plan compared to Western patients?
Tissue character matters more than ethnicity, but there are tendencies. Asian patients often present with firmer, thicker skin and a smaller base, which can hold a lift well but also shows scars differently, so scar protocol matters. Western patients more often have larger, heavier breasts with looser skin that may need an anchor pattern. A good surgeon plans around your measured skin laxity, breast volume, and base width, not a generic ethnic template. The Korean approach is conservative, aiming for a natural, stable shape rather than maximum projection.
What is the recovery downtime for a Korean breast lift?
A surgical bra is worn for about 6 weeks. Desk work resumes in 2 to 3 weeks, and you avoid lifting and overhead reaching for several weeks. Scar management starts around week 6, once incisions have sealed. Swelling settles over 6 to 8 weeks, and the final shape and scar maturation take 6 to 12 months. For an international patient, a stay of around 7 to 10 days covers the suture check and early wound review before flying home, with remote follow-up afterward.
How long does a breast lift last?
A lift resets your starting point, but gravity, aging, weight changes, and future pregnancy still act on the tissue over time. A well-planned mastopexy with a stable internal support and good skin quality can hold a pleasing shape for many years, often a decade or more, before any touch-up is considered. The biggest accelerators of recurrence are large breast weight, very thin skin, significant weight fluctuation, and pregnancy after surgery. This is why surgeons often advise lifting after childbearing is complete.
What anesthesia is used and how long should I stay in Seoul?
A Korean breast lift is performed under IV sedation. Plan a stay of roughly 7 to 10 days so the clinic can check sutures, review early healing, and confirm you are stable before a long flight. After you return home, the clinic handles remote follow-up through messaging and photo review. If you are weighing where to have this done, the most important safeguard is a surgeon who grades your sagging before recommending anything, and you can start that conversation directly with the team at Link Plastic Surgery. Always confirm before booking who manages your aftercare once you leave, what the scar protocol is, and how a revision would be handled if needed.