The Patient Who Comes to Seoul for Revision Rhinoplasty Is Almost Never on Their First Surgery
Walk into a senior revision rhinoplasty consultation in Gangnam and ask the surgeon how foreign patients usually find them. The answer is the same across most established clinics — by the time someone is flying internationally for nose surgery, they are almost always on their second or third procedure, not their first. The typical foreign primary rhinoplasty patient still goes to a local surgeon. The foreign revision patient flies to Korea.
This pattern was not always true. Ten years ago, revision rhinoplasty travel was dominated by Istanbul (for Middle Eastern patients) and Beverly Hills (for North American patients). Korea was a Korean-patient market. The shift over the past five to seven years has been driven by a specific combination — Korean surgeons’ technical comfort with cartilage-graft-heavy reconstruction, the comparatively lower cost relative to U.S. revision pricing, and the fact that the Korean clinic ecosystem has built up enough international-patient infrastructure to handle the multi-week stays that revision cases require.
This guide explains why Korean revision rhinoplasty became the default for foreign patients, what makes the procedure technically harder than primary rhinoplasty, what the recovery actually looks like (it is meaningfully longer than primary), what it costs, and how to verify that a clinic is genuinely set up for revision rather than simply willing to attempt it.

- Most foreign revision rhinoplasty patients in Seoul are on their second or third surgery — and the procedure is technically harder than primary in ways that change the surgical plan, recovery, and cost.
- Korean revision rhinoplasty almost always uses autologous cartilage (your own — usually rib, sometimes ear, occasionally septum if any usable cartilage remains). Implants are avoided in revision when possible because the previous surgery often left scar tissue or thinned skin that makes implant rejection risk higher.
- Recovery is longer than primary — visible swelling resolves over 3–6 months instead of 2–3 for primary, and the final settled shape often is not visible until 12–18 months post-op (compared to 6–12 for primary on Asian patients, 6 for Western patients).
- Korean prices: KRW 9M–15M for revision (USD 6,700–11,200) versus USD 12,000–25,000 in the U.S. and AUD 15,000–28,000 in Australia.
- The most common reasons foreign patients fly to Seoul for revision: contracted nose (“short-nose deformity”) from over-reduced first surgery, dorsal hump recurrence, tip asymmetry, breathing problems from previous over-narrowing, implant complications (extrusion, capsular contracture, infection).
- Plan for a longer Seoul stay — 14 days minimum, ideally 21 days — because revision cases need more in-person follow-up than primary cases do.
- Not every Korean rhinoplasty surgeon does revision well. The skill set is a subset of primary rhinoplasty skill, and clinics that publish revision-specific case galleries are the ones to filter to.
Why Korean Revision Rhinoplasty Became the Default for International Patients
The Korean shift to becoming a global revision-rhinoplasty hub did not happen because Korean primary rhinoplasty got better (it has been excellent for over two decades). It happened because three structural factors lined up over the past five to seven years.
Factor 1 — Cartilage-graft heavy training
Korean primary rhinoplasty has historically been more cartilage-graft-heavy than U.S. or European primary rhinoplasty, because Asian noses typically need more dorsum augmentation and tip projection than Western noses do. The result is that the average Korean rhinoplasty surgeon has handled significantly more cartilage harvesting and grafting cases than the average U.S. surgeon by the time both reach senior level.
That technical comfort with cartilage transfers directly to revision work. Revision rhinoplasty almost always requires rebuilding structure that the previous surgery removed or distorted, and the rebuilding is done with cartilage. Surgeons who already do this routinely have an advantage over surgeons who built primary practices around suture-based tip refinement.
The companion piece on Korean primary rhinoplasty for Asian and Western patients covers why Korean surgeons standardized on the cartilage-additive approach in the first place — that same training pipeline produces the revision specialists.
Factor 2 — Cost differential vs U.S./Australia
Revision rhinoplasty in the U.S. typically runs USD 15,000 to 25,000 with a senior surgeon, sometimes higher. Australian pricing is comparable or higher. Korean revision pricing at established Gangnam clinics typically runs USD 6,700 to 11,200 — a meaningful enough gap that international travel costs are absorbed.
The cost gap is bigger for revision than for primary precisely because revision is a senior-surgeon-only procedure. U.S. and Australian senior surgeons charge premiums for revision that Korean surgeons do not, partly because the Korean cosmetic surgery market is more competitive and partly because Korean revision specialists treat revision volume as part of their practice mix rather than as a specialty premium.
Factor 3 — International-patient infrastructure
The third factor is the part nobody writes about. Korean cosmetic surgery clinics built English-speaking patient coordinator infrastructure during the 2015 to 2020 medical-tourism wave, and that infrastructure is now mature enough to handle revision cases — which need more communication touchpoints than primary cases. A revision patient typically has a video consultation 2 to 4 weeks before surgery (to review prior op notes, prior photos, and plan the rebuild), an in-person consultation on arrival, the surgery, an extended follow-up cadence (day 3, day 7, day 14, day 21), and a remote follow-up protocol for the first 12 months.
That coordination is genuinely difficult. Clinics that built it well during the primary rhinoplasty boom now use it as a competitive advantage for revision cases — and the foreign patients who succeed in Seoul revision are typically the ones who arrived at clinics with that infrastructure rather than at clinics doing revision as a side offering.
What Makes Revision Technically Harder than Primary
Revision rhinoplasty is the same anatomical structure as primary, but the surgical environment is fundamentally different. Three differences drive the technical difficulty.
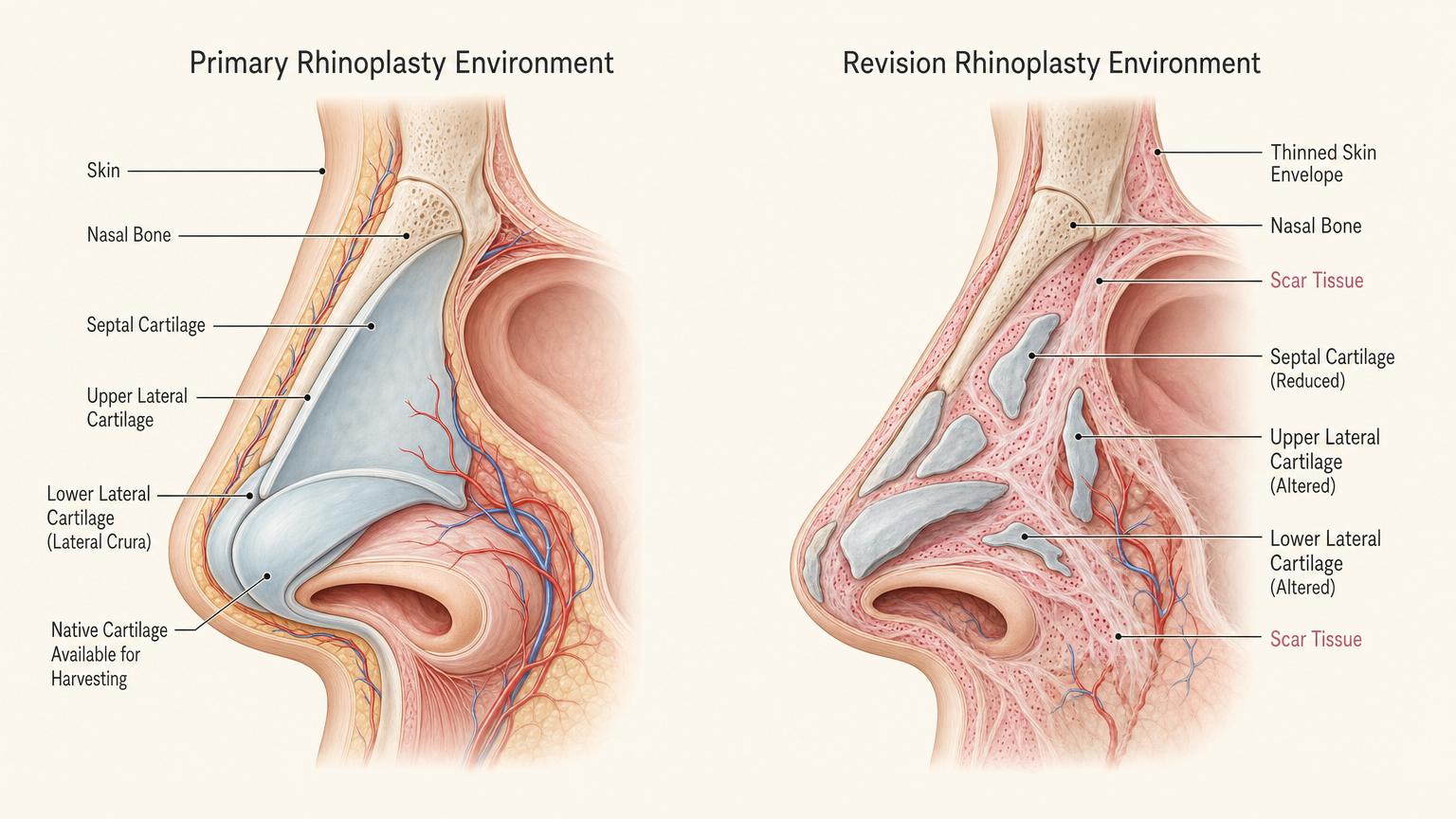
Difference 1 — Scar tissue from the previous surgery
Every primary rhinoplasty leaves scar tissue. Twelve months later that scar tissue has matured into dense fibrous bands that distort surgical planes and make every cut harder than it would have been on virgin tissue. The revision surgeon spends the first 30 to 60 minutes of surgery just clearing scar tissue before reaching the actual structural work.
This is why revision surgical times are typically 1.5 to 2 times longer than primary surgical times. It also drives the higher complication rate — even for senior surgeons, revision has a higher rate of asymmetric healing because the scar tissue distribution is rarely symmetric.
Difference 2 — Cartilage depletion
The previous surgery used some of the patient’s available cartilage. Septal cartilage may already have been harvested. Ear cartilage may already have been used for tip support. The revision surgeon often cannot use the same donor sites the primary surgeon used.
This is why Korean revision rhinoplasty almost always involves rib cartilage harvesting. Rib (costal) cartilage is structurally stronger than septal or ear cartilage and is available in larger volumes than either. The trade-off is a small chest scar (typically 3–4 cm, hidden in the bra line for women) and a slightly longer surgical time. Korean revision surgeons consider the rib harvest a standard part of revision, not an optional add-on.
Difference 3 — Thinned skin envelope
Each rhinoplasty thins the overlying nasal skin slightly. By the time a patient is on their second or third surgery, the skin is meaningfully thinner than at primary. This matters because thin skin shows underlying cartilage irregularities clearly — what would have been an invisible imperfection on virgin skin becomes a visible bump on revision skin.
The revision surgeon compensates by being more conservative with cartilage edges (smoothing rather than building) and by sometimes using a thin layer of fascia or processed cellular dermal matrix to cushion the cartilage from the skin. This is a level of technical detail most primary surgeons rarely handle, and it is one of the reasons revision skill is a subset of primary skill rather than an extension of it.
The Korean Revision Plan — Cartilage, Approach, Timeline
Once the surgeon has assessed the previous surgery and the current state of the nasal anatomy, the revision plan follows a fairly standardized Korean protocol.

Cartilage source — rib first, ear second, septum if available
The default Korean revision approach harvests rib cartilage as the primary structural material. The harvest is done through a 3 to 4 cm incision near the lower border of the breast (for women) or in a similar discrete chest location (for men). The cartilage is processed (carved, shaped, sometimes diced) before grafting into the nasal structure.
Ear cartilage is added if needed for softer, more flexible grafts in tip refinement or for caudal septal extension. Septal cartilage is used only if the previous surgery did not deplete it — many revision patients have no usable septal cartilage left.
Open vs closed approach
Almost all Korean revision rhinoplasty is performed open — meaning a small incision across the columella (the strip of tissue between the nostrils) is added to give the surgeon full visibility of the underlying structure. The columellar scar fades to invisible by month 3 to 6.
Closed (endonasal) revision is technically possible but rare in Korea because the visibility tradeoff is severe in a scar-tissue environment. Senior revision surgeons almost universally use open.
Timeline
The surgical procedure itself takes 4 to 6 hours under IV sedation, compared to 2 to 4 hours for primary. The patient leaves the clinic with a dorsal splint, internal nasal stents (removed at day 3 to 5), and a small chest binder over the rib harvest site.
Day 1 to Day 7 — splint and bruising

The first week of revision recovery is similar to primary recovery in terms of nasal swelling and bruising, but with the added discomfort of the rib harvest site. Most patients describe the rib site as more uncomfortable than the nose during the first 5 days — sharp pain on deep breathing, tenderness when laughing, careful sleeping position. The pain medication regimen is longer than primary (5 to 7 days versus 3 to 5).
Day 7 to Day 21 — extended Seoul stay
The dorsal cast comes off at day 7. The columellar incision sutures are removed at day 7 to 10. The chest binder stays on for 14 to 21 days depending on the rib harvest size. Most foreign revision patients stay in Seoul through at least day 14 and ideally day 21 to allow proper in-person follow-up at the day-7 cast removal, the day-14 swelling check, and the day-21 final review before international travel.
This is where revision differs most from primary — the extended in-person follow-up cadence. A primary rhinoplasty patient flying out at day 7 is a normal scenario. A revision rhinoplasty patient flying out at day 7 is a clinic accepting a higher complication risk. Plan accordingly.
Month 3 to Month 18 — slow settling
Revision swelling resolves more slowly than primary swelling. The 80% point is around month 6 instead of month 1. The 90% point is around month 12 instead of month 3. The truly final settled shape often is not visible until month 18, particularly for thicker-skinned Asian patients.
This longer timeline is why revision satisfaction surveys typically wait until 18 months post-op rather than 12 months. The patient who is not happy at month 6 is usually happy at month 12, and the patient who is not happy at month 12 is sometimes happy at month 18. Patience is a real component of the revision recovery curve.
What It Costs and How to Find a Real Korean Revision Specialist
Revision pricing is more variable than primary pricing because the technical complexity ranges widely depending on what the previous surgery did.
| Procedure | Korea (KRW) | USD | U.S. comparable | Australia comparable |
|---|---|---|---|---|
| Minor revision (single-issue, partial) | 7M – 9M | $5,200 – $6,700 | $10,000 – $15,000 | AUD 12,000 – 18,000 |
| Standard revision (full rebuild, rib graft) | 9M – 14M | $6,700 – $10,400 | $15,000 – $25,000 | AUD 18,000 – 28,000 |
| Complex revision (3rd+ surgery, severe scar) | 14M – 20M | $10,400 – $15,000 | $22,000 – $35,000 | AUD 25,000 – 40,000 |
| Implant removal + cartilage rebuild | 10M – 15M | $7,400 – $11,200 | $16,000 – $26,000 | AUD 19,000 – 30,000 |
Established Gangnam clinics that publish surgeon-specific revision galleries — including the dedicated Link Plastic Surgery revision rhinoplasty page — sit in the middle of these ranges. Cheaper revision quotes from app-based platforms or generic medical-tourism agencies typically exclude the rib harvest fee, exclude the extended in-person follow-up sessions, or assume a junior surgeon rather than a senior revision specialist. Revision is the procedure where the cheapest option costs the most over a 3-year window once you factor in the higher complication rate at non-specialist clinics.
How to verify a revision specialist

A few specific questions separate genuine Korean revision specialists from generalists who accept revision cases:
- Does the clinic have a separate published revision case gallery (not bundled with primary cases)? Generic clinic galleries that lump primary and revision together are a sign that revision is not a focused practice area. Several Gangnam clinics — including Link Plastic Surgery — publish revision-specific galleries that allow this verification.
- Is rib cartilage harvest part of the standard quoted fee, or billed as an add-on? In a real revision practice it is included. In clinics treating revision as a side offering, it is sometimes offered as an upsell — which is a yellow flag.
- Does the consultation include a review of your prior operative notes (or at least your prior photos taken at multiple time points)? A revision plan made without seeing what the previous surgeon did is a plan made on guesswork.
- What is the in-person follow-up cadence for international revision patients? “Day 3, day 7, day 14, day 21” is the standard at established revision practices. “Day 7 and then fly home” is a generalist clinic.
- What is the surgeon’s stated revision rate (the percentage of their own primary cases that subsequently need revision)? Senior revision specialists typically know this number and quote it openly. Surgeons who deflect this question are signaling something.
If a clinic answers most of these clearly without you having to push for specifics, that is a clinic genuinely set up for revision. If the answers are vague or shift to “you can ask in the consultation,” that is the signal to look elsewhere.
Recommended for Your Recovery
Products patients commonly use during the extended revision rhinoplasty recovery window — same items routinely included in the post-op kits Seoul clinics hand out at discharge.
- Arnica Montana Tablets — start 3 days before surgery to reduce bruising along the under-eye area and around the rib harvest site. Check price on Amazon
- Bromelain Supplement (500mg) — natural anti-inflammatory commonly recommended by Korean clinics for the longer revision swelling timeline. Check price on Amazon
- Silicone Scar Sheets — cut to size and apply along the rib harvest scar from week 3 onward to optimize how the chest scar matures. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — lightweight Korean sunscreen for the healing nasal skin from week 2 onward to prevent post-inflammatory pigmentation, particularly important on revision skin which is thinner than primary. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
Frequently Asked Questions
How long after my original rhinoplasty should I wait before revision?
Minimum 12 months. Most Korean revision specialists prefer 18 months. The reason is that swelling and tissue settling continue for up to 18 months even after primary, and what looks like a problem at month 6 sometimes resolves on its own by month 12. A revision performed too early operates on tissue that has not finished healing, which complicates the surgical environment unnecessarily.
Will I definitely need rib cartilage?
For most second or third surgeries, yes. Septal and ear cartilage are usually depleted by the previous surgery, and the structural rebuild needs material that only rib provides in adequate volume. Some minor revisions (single-issue, partial) can be done with ear cartilage alone, but the surgeon decides this on examination — not on patient preference.
How long do I need to stay in Seoul?
Minimum 14 days, recommended 21 days. The follow-up cadence is denser than primary (day 3, 7, 14, 21) and the early decisions on sutures, splint timing, and rib site healing benefit from in-person visits. Patients flying out at day 7 are accepting a higher complication risk.
How visible is the rib cartilage scar?
3 to 4 cm scar in the lower breast crease (for women) or a similar discrete chest location (for men). After 6 months it fades to a thin pale line that is invisible under bras, swimwear, or normal clothing. From any standing angle it is not visible. Up close in good light it is detectable as a thin pale line.
Is there a higher complication rate for revision than primary?
Yes. Even in expert hands the asymmetric healing rate is higher because the underlying scar tissue is rarely symmetric. Korean senior revision specialists typically quote 5–10% touch-up rates at 18 months, compared to 2–5% for primary. Revising a revision is harder than the original revision was, so picking the right surgeon for the rebuild matters more than for primary.
Can I see Korean and non-Korean revision cases in the surgeon’s gallery?
You should be able to. Top revision practices show both. The companion primary rhinoplasty page covers the same surgeon’s primary work — comparing primary and revision galleries from the same surgeon is the most reliable verification step before booking.
What if my original surgery was an implant that failed?
Implant removal plus cartilage rebuild is a specific revision pattern with its own protocol. The implant is removed, the capsule (scar pocket around the implant) is excised or partially preserved depending on its condition, and the structural support is rebuilt with rib cartilage. Recovery is similar to standard revision but with slightly more dorsal swelling because the implant pocket needs to fill in and contract over months 3 to 12.
Is revision with no chest scar possible?
Sometimes — for minor revisions where ear cartilage is sufficient. For most second-surgery cases, the answer is no. If a clinic promises rib-free revision for a complex case, that is a yellow flag. The structural material has to come from somewhere, and with septal cartilage depleted and ear cartilage limited, rib is the realistic source.