The patient had spent weeks in online forums and arrived convinced she had to pick a side. Silicone or your own cartilage. Implant or natural. She had read horror stories about implants and miracle stories about rib cartilage, and she wanted the surgeon to tell her which camp was right. He listened, examined her nose, and gave her an answer she had not expected: both. Her bridge would take an implant, her tip would take her own cartilage, and that combination was not a compromise but the standard. The false choice she had been agonizing over did not really exist. The consultation at Link Plastic Surgery often starts by dismantling that exact misconception.

Rhinoplasty material is one of the most argued-about topics among foreign patients researching Korean nose surgery, and most of the argument rests on a misunderstanding. People treat silicone implants and their own cartilage as opposing philosophies, as if a good surgeon chooses one and rejects the other. In reality they do different jobs in different parts of the nose, and the overwhelming majority of Korean rhinoplasty uses a combination. Understanding what each material is actually for is the difference between an informed decision and a forum-fueled panic.
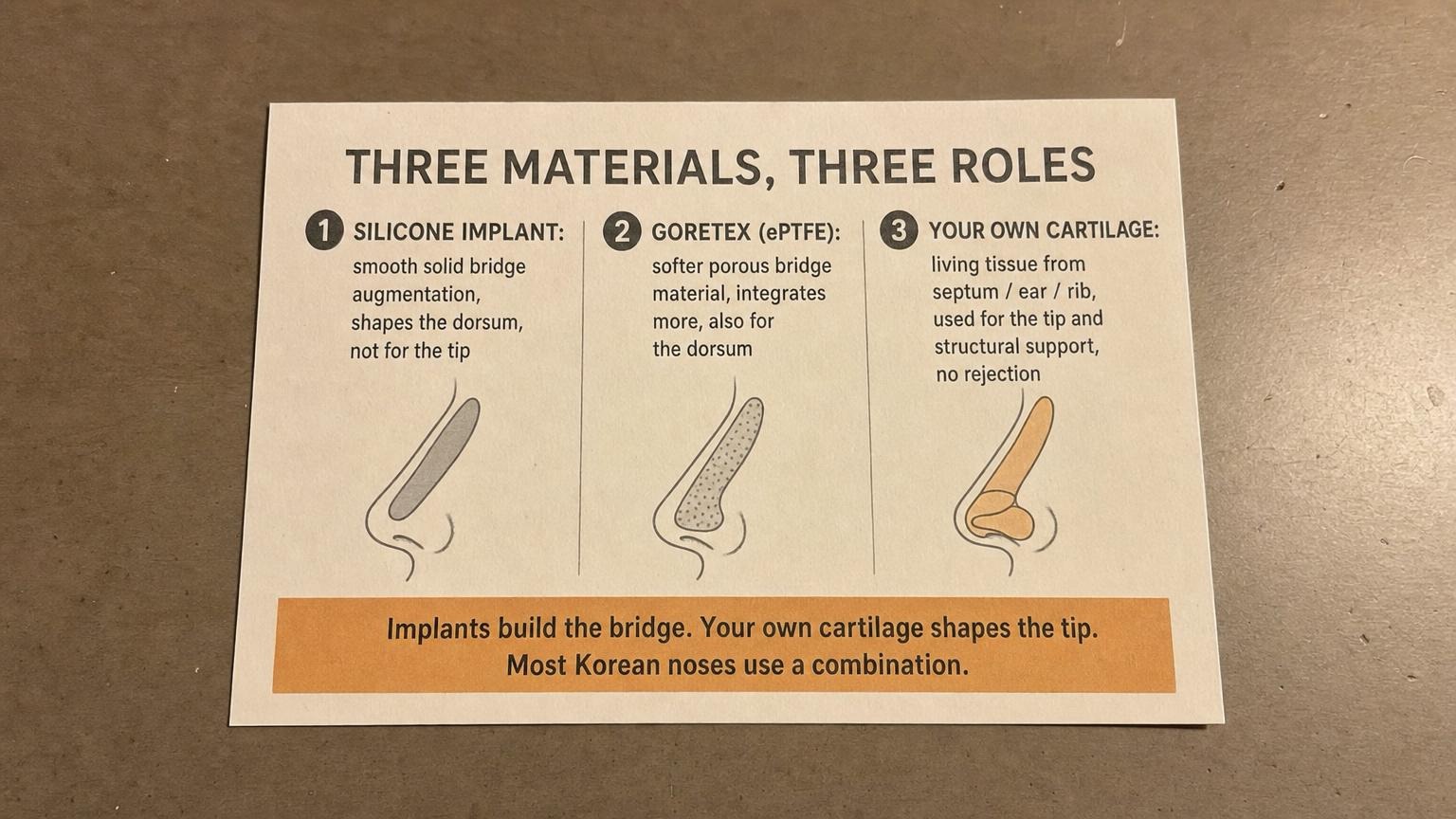
Three Materials, Three Different Roles
There are three materials that come up in almost every Korean rhinoplasty discussion, and each has a specific job. The mistake is comparing them as if they were interchangeable, when they are really specialists.
Silicone implants are smooth, solid pieces used to augment and shape the bridge, the dorsum of the nose. They give a clean, predictable line to the bridge and have decades of use behind them. Goretex, a softer porous material, also augments the bridge but integrates more with the surrounding tissue, which some surgeons prefer for a more natural feel. Both are bridge materials. Neither is appropriate for the tip.
Your own cartilage is the third material, and it is fundamentally different because it is living tissue from your own body. It is used for the tip and for structural support, and because it is yours, there is no question of rejection. The detailed surgical context is covered in our guide to Korean rhinoplasty. The key idea to hold onto is simple: implants build the bridge, your own cartilage shapes the tip, and most noses need both.
Where Your Own Cartilage Comes From
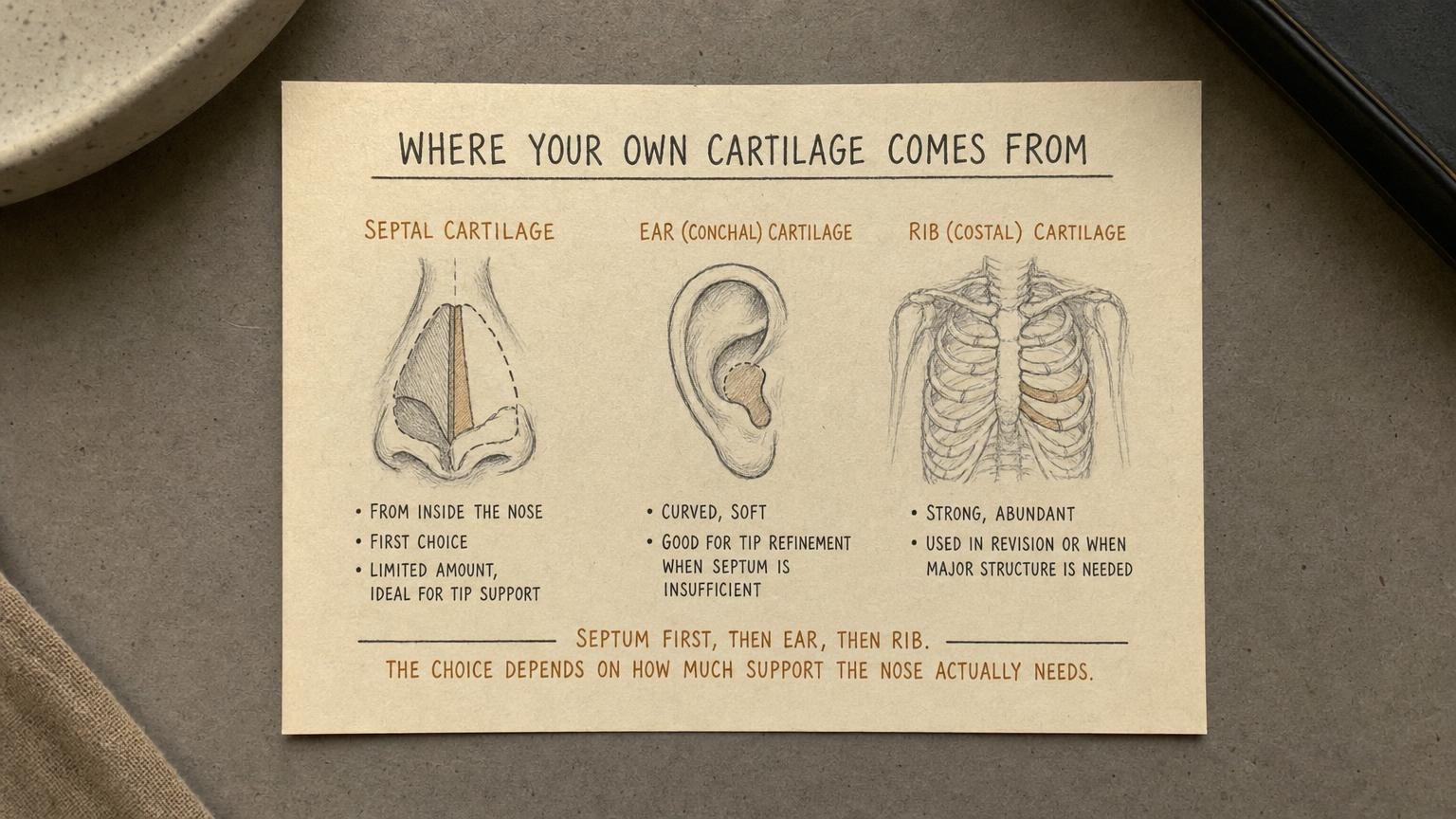
When surgeons talk about using your own cartilage, they are drawing from one of three sources, and the choice follows a clear logic based on how much support the nose actually needs.
Septal cartilage, taken from the wall inside the nose, is the first choice. It is straight, strong, ideal for tip support, and harvesting it does not create a visible donor site. The limitation is quantity; there is only so much septal cartilage available, especially in a smaller nose. When the septum cannot supply enough, ear cartilage is the next option. It is curved and soft, which makes it well suited to refining the tip, and the small donor scar behind the ear is hidden. For cases that need substantial structure, particularly revisions, rib cartilage provides a strong and abundant supply, though harvesting it is a larger undertaking. The order is consistent: septum first, then ear, then rib, matched to the structural demand of the nose. This logic matters most in Korean revision rhinoplasty, where the original cartilage is often depleted.
Why Most Korean Noses Use Both
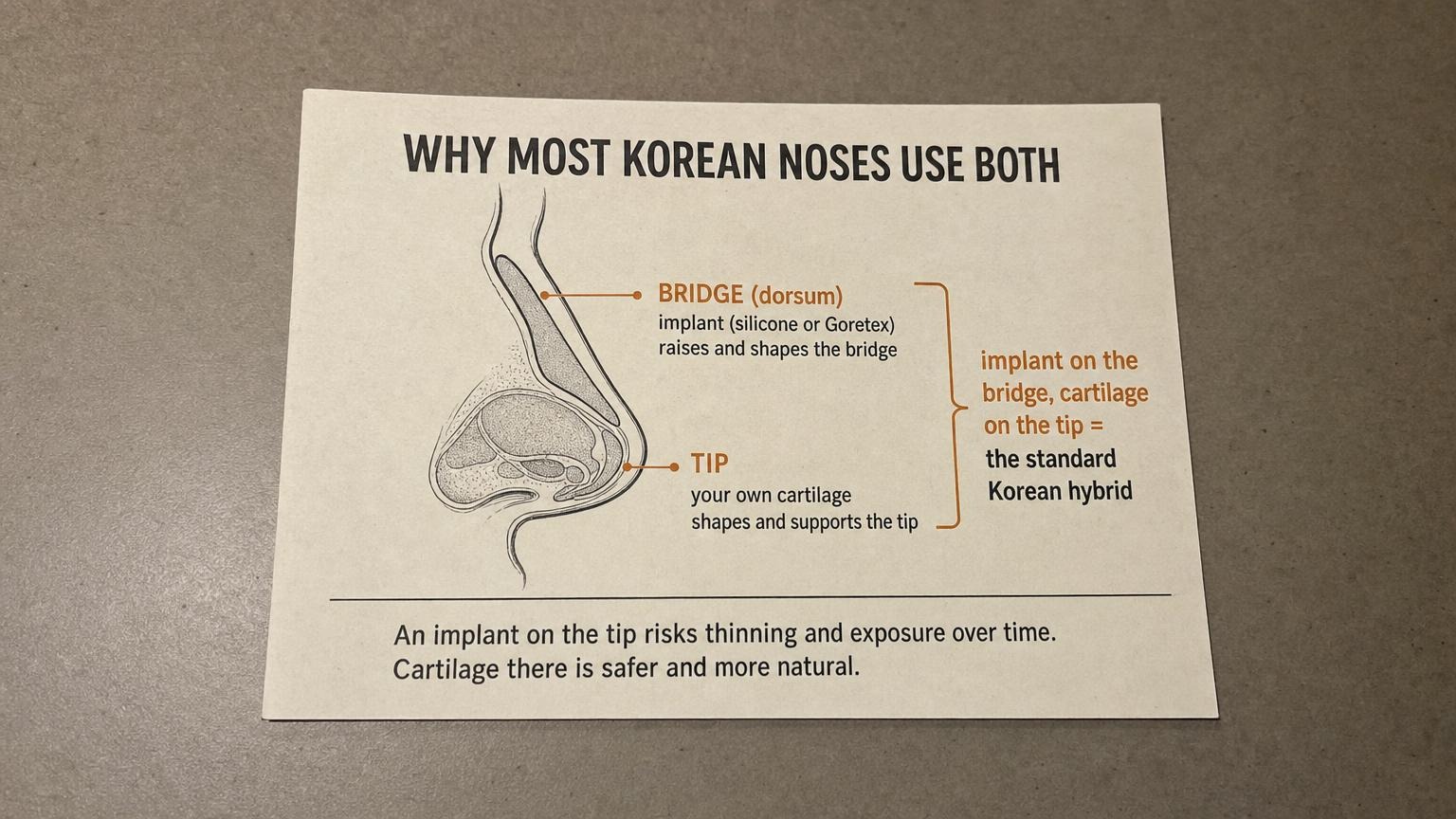
The central insight that dissolves the implant-versus-cartilage debate is anatomical. The bridge and the tip have different requirements, so they are best served by different materials.
Recommended for Your Recovery
Products commonly used before and after Korean rhinoplasty implant vs cartilage materials — same items routinely recommended in the recovery instructions Seoul clinics hand out at discharge.
- Arnica Montana Tablets — start 3 days before facial surgery to reduce bruising in the treated area. Check price on Amazon
- Silicone Scar Sheets — for procedures with visible incisions, apply from week 3 onward to support scar maturation. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — daily Korean SPF 50+ to protect freshly treated facial skin. Check price on Amazon
- COSRX Advanced Snail 96 Mucin Power Essence — Korean snail mucin essence to support the post-procedure skin barrier. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
The bridge needs a smooth, stable augmentation to create a clean profile line, and an implant does this predictably and well. The tip, however, is covered by thinner, more mobile skin and sits at the most exposed point of the nose. Putting a hard implant at the tip risks the material thinning the skin over time and, in the worst case, becoming visible or extruding. This is precisely why experienced Korean surgeons use cartilage at the tip: it is softer, it is living tissue, and it integrates safely where an implant would be a long-term liability. So the standard Korean approach places an implant on the bridge and the patient’s own cartilage on the tip. This is not a hedge or a compromise; it is the combination that gives the most natural and durable result. The patient agonizing over which side to choose was solving a problem that good surgical practice had already solved.
Which Material Fits Which Nose
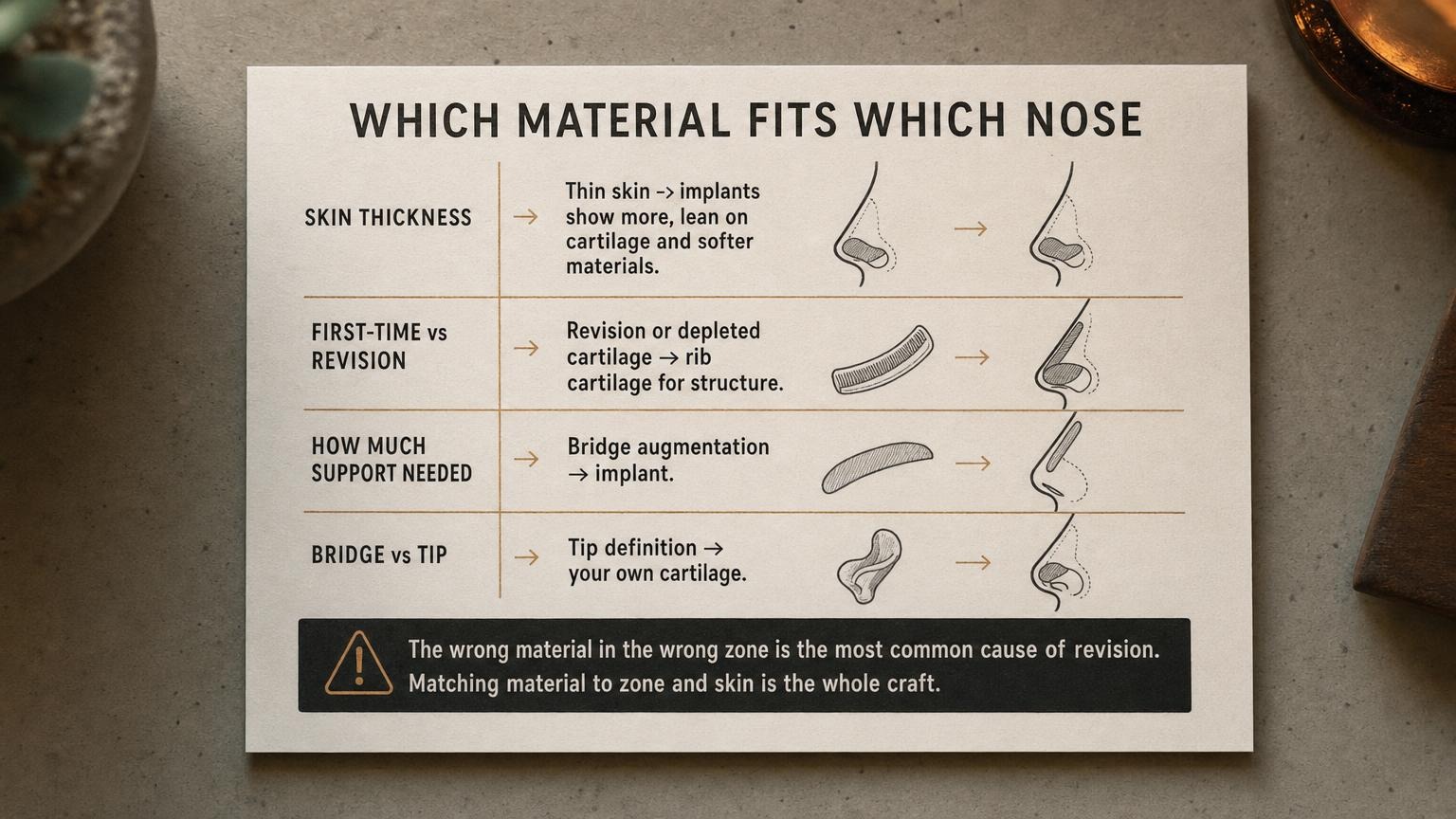
While the bridge-implant tip-cartilage combination is the default, the specifics are tailored to the individual nose, and a few factors drive the decision.
Skin thickness is one of the most important. Thin skin shows everything underneath it, so in a thin-skinned nose an implant on the bridge can become more visible over time, and surgeons lean toward softer materials and more cartilage to camouflage the structure. Thicker skin is more forgiving. Whether the surgery is a first-time procedure or a revision matters too; revisions often involve scar tissue and depleted cartilage, which is when rib cartilage becomes necessary to rebuild structure. And the basic division holds throughout: bridge augmentation calls for an implant, tip definition calls for your own cartilage. The most common reason patients end up needing revision is the wrong material in the wrong zone, an implant pushed into tip work it was never suited for, or inadequate structural support. Matching material to zone and to skin is the actual craft of rhinoplasty. The same matching logic extends to related procedures like Korean alar reduction when the nostrils are addressed in the same operation.
Cost and How to Verify the Plan
Pricing varies with complexity and materials. A primary Korean rhinoplasty using an implant for the bridge and septal or ear cartilage for the tip typically runs in a mid-range that reflects a standard combination procedure. Cases requiring rib cartilage, particularly revisions, cost more because the harvest and reconstruction are more involved. These figures are generally below the equivalent in the United States or Australia, which is part of why nose surgery anchors so many Seoul trips. The broader context of facial balance, since the nose is never planned in isolation, is covered across our Korean facial procedure guides.
Before committing, five questions tell you whether a surgeon is planning carefully or applying a template. What material is planned for the bridge, and what for the tip, and why each? If an implant is used, how is the tip being protected with cartilage? Which cartilage source is planned, and what is the backup if the septum is insufficient? How does your skin thickness affect the material choice? And if this is a revision, is there enough cartilage left, or is rib cartilage needed? A surgeon who answers these clearly, zone by zone, is planning your nose specifically. One who just says implant or just says all cartilage without explaining the zones is applying a formula. For trip-planning details, our broader resources at Link Plastic Surgery cover the practicalities for international patients.
Frequently Asked Questions
1. Is silicone or my own cartilage better for rhinoplasty?
Neither is better in the abstract because they do different jobs. Silicone implants augment the bridge predictably, while your own cartilage shapes and supports the tip safely. Most Korean rhinoplasty uses an implant on the bridge and cartilage on the tip together. The question is not which to choose but where each belongs.
2. Are silicone implants dangerous?
Used correctly on the bridge, silicone has a long track record and is considered safe. The problems people read about usually come from misuse, most often placing an implant at the tip where the skin is thin and the material can thin the skin or become visible over time. On the bridge, in a nose with adequate skin, it is a standard and reliable material.
3. Why not use my own cartilage for the whole nose?
For the tip, cartilage is indeed preferred. For the bridge, an implant often gives a smoother, more predictable line, and using cartilage there can require a large amount, sometimes rib cartilage with a bigger donor procedure. Some patients do have all-cartilage rhinoplasty, particularly thin-skinned patients or revisions, but for many a combination is simpler and equally natural.
4. What is the difference between silicone and Goretex?
Both augment the bridge. Silicone is a smooth solid implant that gives a clean predictable line and is easy to remove or revise. Goretex is a softer porous material that integrates more with surrounding tissue, which some find more natural to the touch but harder to remove later. The choice depends on the surgeon’s judgment and the patient’s tissue and goals.
5. Which cartilage source is best?
It depends on how much is needed. Septal cartilage is the first choice because it is strong, straight, and leaves no visible donor site, but quantity is limited. Ear cartilage is next, good for tip refinement. Rib cartilage is used when substantial structure is needed, especially in revisions, at the cost of a larger harvest. The order is septum, then ear, then rib.
6. Does skin thickness change the material choice?
Yes, significantly. Thin skin reveals whatever is underneath, so surgeons lean toward softer materials and more cartilage to avoid the structure showing over time. Thicker skin hides the structure better and is more forgiving of implants. Assessing skin thickness is a key part of choosing materials correctly.
7. I had an implant before and want it removed. What replaces it?
That is a revision, and the replacement depends on what the nose needs structurally. Often the answer is cartilage, and if the septum and ear cannot supply enough, rib cartilage is used to rebuild the bridge and support the tip. Revision planning hinges on how much usable cartilage remains, which is why an honest assessment matters.
8. Will an implant look unnatural?
On the bridge, in a nose with adequate skin and with the tip handled by cartilage, a well-placed implant looks natural and follows the Korean preference for a balanced, not overly high, profile. Unnatural results usually come from an implant that is too large, too high, or wrongly placed at the tip, not from implants as such.
9. Does Asian and Western rhinoplasty use materials differently?
The principles are the same, but the typical goals differ. Asian rhinoplasty more often augments a lower bridge, where implants are commonly used, while Western noses more often involve reducing a hump or refining structure. The bridge-implant tip-cartilage logic applies broadly, adjusted to the starting anatomy and the goal.
10. How do I plan rhinoplasty material choices as an international patient?
Have a consultation that specifies the material for the bridge and the tip separately, with the reasoning, and confirm the cartilage source and a backup plan. For a revision, confirm there is enough cartilage or that rib is planned. For scheduling and trip-planning details, visit Link Plastic Surgery’s official website.