Korean Elastic Tummy Tuck for Postpartum Diastasis Recti: A Foreign Mother’s Guide

Foreign mothers searching “Korea tummy tuck cost” are almost never asking the question they think they are asking. They have a postpartum belly that has not flattened despite a year or more of consistent exercise, they have read marketing language about Korean body contouring, and they imagine a single fast procedure — usually some version of stronger liposuction — that will give them their pre-pregnancy abdomen back. The Korean surgical consultation tells a different story. There are three separate problems hiding inside one postpartum belly: subcutaneous fat, separated rectus abdominis muscles (diastasis recti), and a stretched skin envelope with a deformed belly button. Each requires a different surgical answer. The Korean elastic tummy tuck addresses all three in one integrated operation. This guide explains what foreign mothers misunderstand about the procedure, what Seoul clinics actually do for postpartum bodies, why liposuction alone almost never solves the problem mothers came in to fix, and how clinics — including Link Plastic Surgery — sequence the layered correction across one surgical session.
Section 1 — What Foreign Mothers Are Actually Asking When They Search “Korea Tummy Tuck”
The search pattern is consistent across the foreign mothers who arrive in Seoul for consultation. They are typically 18 months to 5 years postpartum. They have lost the pregnancy weight or come close to it. They have been doing core workouts, planks, pilates, sometimes physical therapy, for at least a year. And the lower abdomen still bulges. They Google “Korea tummy tuck cost” expecting to find a faster, cheaper version of the United States or Australian mommy makeover. What they actually need is a different surgical conversation than the one they prepared for.
The Three Problems Hidden Inside One Postpartum Belly
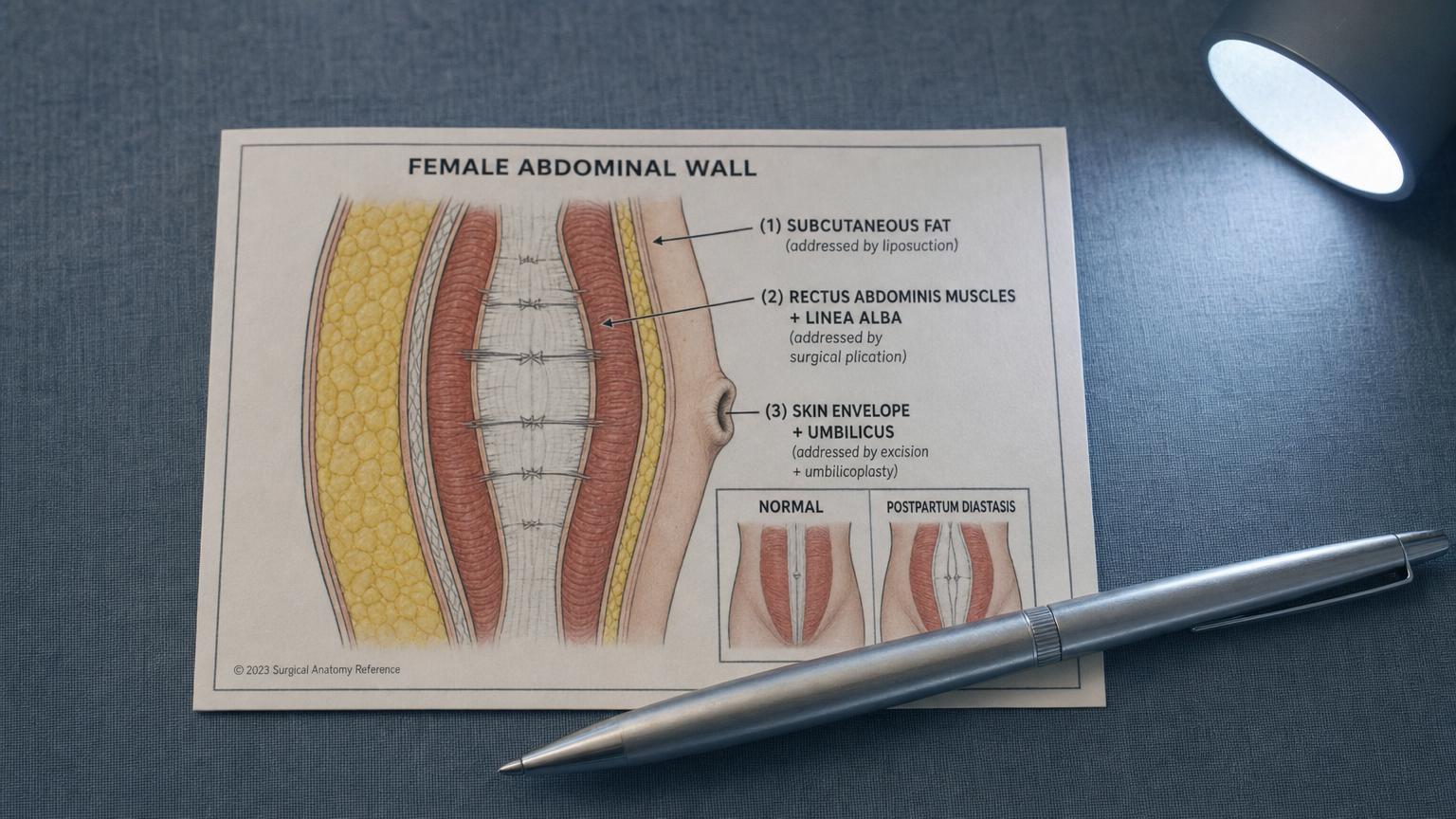
The postpartum abdomen is rarely one problem. It is usually three problems stacked on top of each other, and the foreign patient sees only one.
Problem 1 — Subcutaneous fat. The layer of fat sitting between the skin and the abdominal wall muscles. This is what foreign mothers think the whole problem is. Liposuction addresses this layer — micro-cannula technique, 2 to 3 mm, deliberate preservation of the subdermal 5 mm layer, the conservative Korean protocol covered in detail in the Link Plastic Surgery liposuction page. Removing subcutaneous fat changes the apparent thickness of the abdomen but does not change anything underneath.
Problem 2 — Diastasis recti. The two halves of the rectus abdominis muscle — the muscle that creates the visible “six-pack” line in lean individuals — are held together at the midline by a strip of connective tissue called the linea alba. During pregnancy, the growing uterus stretches this connective tissue laterally, sometimes by 5 cm or more at the widest point. After delivery, in roughly two-thirds of women, the linea alba does not fully return to its pre-pregnancy width. The result is a soft midline gap that can be felt when palpating the abdomen and that often shows as a visible vertical doming or bulge when the core is engaged (sitting up from a flat position, for example). Diastasis recti is not a fat problem and not a skin problem. It is a structural problem of separated muscles. Only surgical plication — suturing the two sides of the rectus back to the midline — closes it.
Problem 3 — Loose skin and a stretched belly button. Pregnancy stretches the skin envelope of the abdomen substantially, and the dermis loses elasticity in the process. After delivery and weight normalization, the skin often does not retract fully, and the belly button — which is held in place by a stalk anchoring it to the abdominal wall — frequently elongates, deforms, or develops a hooded appearance. Skin laxity is not addressed by liposuction (removing fat from under loose skin makes the skin looser, not tighter) and not by diastasis repair alone. Only surgical excision of the redundant skin, combined with neo-umbilicoplasty — repositioning the original belly button through a new opening in the tightened skin — produces a flat envelope with a natural belly button position.
Why One Procedure Cannot Replace Another
This is the conversation foreign patients struggle with the most. They want to believe that strong liposuction will deliver the result they want. Korean surgeons routinely explain why it will not, and the explanation has a specific anatomical form. Liposuction on a diastasis recti abdomen will remove the fat, yes, but the bulging muscle gap remains visible — the patient gets a thinner belly with the same midline dome, sometimes more obvious than before because there is less fat masking it. Liposuction on a stretched skin envelope makes the loose skin worse — there is now less volume underneath for the skin to drape over, and the loose envelope hangs more obviously. A tummy tuck without integrated liposuction tightens the front of the abdomen but leaves the flanks and upper abdomen unsculpted, producing a contour mismatch where the flat front meets the rounder sides.
This is why the layered correction matters. The Korean elastic tummy tuck integrates all three layers in one operative session, so the abdominal wall is rebuilt as a single tensioned unit. The post-operative contour is continuous from flank to flank, the midline is flat without bulging, the skin envelope is taut without hanging, and the belly button looks natural rather than constructed.
The Korean Clinical Consultation Pattern
What happens in a Seoul consultation for a postpartum patient is different from what foreign patients expect, and the difference is anatomical separation. The surgeon does not just look at the belly and propose a procedure. The surgeon performs a small set of diagnostic checks that separate the three layers.
The belly button finger test is the first check, and most foreign patients have never been shown this. The patient lies flat on the exam table with knees bent. The surgeon asks the patient to place one hand behind the head, lift the head slightly off the table — just enough to engage the abdominal muscles — and the surgeon palpates the midline above, at, and below the navel with two fingers pressed vertically into the abdomen. The width of the gap between the two halves of the rectus muscle is measured in finger-widths. Under 1 finger-width (about 1 cm) is normal. 2 finger-widths is a mild diastasis that may or may not need surgical repair depending on patient priorities. 3 or more finger-widths is a significant diastasis that exercise will not close and that benefits from surgical plication.
The skin pinch test is the second check. The surgeon pinches a fold of abdominal skin between thumb and forefinger, evaluates how thick the fold is, how readily it springs back when released, and whether the underlying tissue can be moved independently. Thick, slow-recoiling skin indicates a stretched envelope that will not retract on its own. Thin, springy skin indicates good elasticity that may not need excision.
Visual evaluation of the fat layer is the third check — sometimes supplemented with abdominal ultrasound to differentiate subcutaneous from intra-abdominal (visceral) fat. Subcutaneous fat is addressable by liposuction. Visceral fat is not — that is a metabolic and weight-management question, not a surgical one. Foreign patients who arrive substantially above their goal weight are gently redirected to lose the weight first and return for surgical contouring after.
Why Foreign Patients Arrive Misinformed
International clinic websites tend to blur the three procedures into “mommy makeover packages” for marketing simplicity. The package typically lists tummy tuck, liposuction, and breast surgery as bundled options, but the descriptions rarely separate diastasis recti repair as its own component — it tends to be folded silently into “abdominoplasty” without explaining what is actually being done structurally. The result is foreign patients who book a “mommy makeover” without understanding which of the three abdominal problems are being addressed.
Korean surgeons unpack the bundle again at consultation, which feels like upselling but is actually anatomical separation. The patient who came in expecting a simple lipo is told that the lipo alone will not fix the midline dome. The patient who came in expecting a tummy tuck without lipo is told that the flanks will look mismatched without integrated sculpting. The honest framing is that the postpartum abdomen needs the procedure to match the problem, and the problem is usually three problems.

Section 2 — The Korean Elastic Tummy Tuck: A Three-Layer Procedure, Not an Upgraded Liposuction
The word “elastic” in the Link PS context refers to the integration of liposuction, rectus plication, skin excision, and umbilicoplasty performed in sequence during one operation. The abdominal wall is rebuilt as a single tensioned unit rather than three separate fixes done at different visits. This is the technical core of why the procedure is named differently from a standard abdominoplasty — not because the underlying surgery is different from abdominoplasty elsewhere, but because the integrated execution is what separates a balanced postpartum result from a partial one.
Layer 1 — The Liposuction Component
The first layer addressed during the operation is the subcutaneous fat layer at the flanks, upper abdomen, and lateral hips. This is performed with the same micro-cannula technique used in standalone Korean liposuction — 2 to 3 mm cannulas, multi-layer aspiration, deliberate preservation of the 5 mm subdermal fat layer to support skin retraction. The volumes are conservative: 200 to 400 ml per flank, 200 to 300 ml across the upper abdomen, modest contouring at the lateral hips. The point is contour balance, not aggressive fat removal — by the time the operation moves to the skin excision phase, the flanks have already been sculpted, so the new contour matches the lateral waistline rather than creating a flat-front-rounded-sides mismatch.
This is where the foreign patient’s liposuction expectations are addressed — but it is the surface layer, not the structural correction. Foreign patients who book hoping that strong lipo will solve the postpartum bulge are addressed at this stage of the procedure, but the structural work is just beginning.
Layer 2 — Rectus Plication (Diastasis Recti Repair)
The structural step that foreign patients did not know they needed. The surgeon makes the horizontal abdominoplasty incision along the bikini line, lifts the skin and subcutaneous fat upward as a flap, and exposes the abdominal wall musculature. The diastasis is now directly visible — the two halves of the rectus abdominis muscle separated along the midline, with the stretched linea alba spanning the gap.
Plication is performed with non-absorbable or long-absorbable sutures placed at intervals along the entire vertical length of the diastasis, from the xiphoid (just below the breastbone) down to the pubis. Each suture brings the two halves of the rectus back to the midline, restoring core wall integrity. The sutures are typically placed in two layers — a deeper layer for structural strength and a more superficial layer for contour. The result is a flat, firm abdominal wall that no longer bulges at the midline when the core is engaged.
This is the step that makes the belly look flat and feel firm rather than just flat. Without plication, even a thin postpartum belly retains the soft, doughy midline that exercise has not been able to address. With plication, the abdominal wall has the firmness it had before pregnancy. Foreign patients consistently report this as the most unexpected positive outcome — they came in for “looking better” and discovered that their core also functions better post-operatively, with less lower back strain and more efficient sit-up and forward-bend mechanics.
Layer 3 — Skin Envelope Correction and Neo-Umbilicoplasty
With the rectus plicated and the abdominal wall reconstructed, the skin flap is pulled downward over the now-flat abdomen. The amount of redundant skin between the navel and the pubis is marked, excised, and the lower edge of the upper flap is sutured to the upper edge of the pubic skin along the bikini-line incision.
The belly button needs a new position, because the old position no longer matches the tightened abdomen. The Korean technique preserves the original belly button rather than constructing a new one from scratch. The original navel — including its stalk that connects it to the abdominal wall — is left in place, and a new opening is cut in the tightened skin flap above it. The original belly button is then drawn up through the new opening and sutured into place. This is neo-umbilicoplasty. The reason for preserving the original is that a constructed belly button typically looks surgical, with visible scarring around a circular or oval opening, while a preserved original retains the natural depth, shape, and hooded appearance that the patient had before pregnancy.
Why This Layered Approach Matters for Postpartum Bodies Specifically
Pregnancy stretches all three layers simultaneously. Fat is deposited in the subcutaneous layer in preparation for breastfeeding. The rectus muscles are separated by the growing uterus. The skin envelope is expanded by the same growth. The three problems are not independent — they happen together, and they need to be corrected together for the result to be coherent.
Correcting only one layer produces partial results that mothers describe as “better but not what I came for.” The liposuction-only result is a thinner belly with the same midline dome. The plication-only result is a firm midline with hanging skin. The skin-excision-only result is a flat envelope with no fat reduction at the flanks. The Korean elastic tummy tuck delivers all three corrections in one operative session, which is why the post-operative contour is continuous and the recovery timeline is one timeline rather than three.
Mini vs Full vs Elastic Korean Variants
A mini tummy tuck addresses only the area below the navel with a shorter horizontal incision; it does not include diastasis repair above the navel, and it does not include belly button repositioning. This is rarely the correct procedure for postpartum patients because postpartum diastasis usually extends above the navel as well, and a mini procedure leaves the upper diastasis unaddressed. The patient gets a flatter lower abdomen with a persistent midline dome above the navel — the partial-result pattern.
A full tummy tuck addresses the full vertical span from xiphoid (lower ribs) to pubis, includes diastasis repair across the full length of the rectus separation, and includes belly button repositioning. This is the appropriate procedure for most postpartum patients with significant diastasis.
The Link PS elastic version emphasizes integrated liposuction sculpting performed in the same operative session as the full tummy tuck. The detail is described on the Link Plastic Surgery elastic tummy tuck page. The integration is what produces the continuous flank-to-flank contour and addresses the lateral waistline that a standalone full tummy tuck without lipo would leave unsculpted.
Section 3 — Diastasis Recti: The Postpartum Problem Foreign Mothers Don’t Know Has a Name
Diastasis recti is the medical term for separation of the two halves of the rectus abdominis muscle along the midline connective tissue called the linea alba. It is one of the most common postpartum changes and one of the least recognized by foreign mothers before they arrive in Seoul for consultation. The condition is often called by other names colloquially — “mommy pooch,” “belly gap,” “abdominal separation” — but the underlying anatomy is the same in every case.
Recommended for Your Recovery
Products commonly used before and after Korean elastic tummy tuck postpartum diastasis recti — same items routinely recommended in the recovery instructions Seoul clinics hand out at discharge.
- Arnica Montana Tablets — start 3 days before body surgery to reduce bruising in the treated zone. Check price on Amazon
- Silicone Scar Sheets — cut to size and apply over incision lines starting week 3 to flatten scar formation. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — daily UV protection on healing scars — sun exposure during the first 6 months drives post-inflammatory pigmentation. Check price on Amazon
- COSRX Advanced Snail 96 Mucin Power Essence — gentle Korean skin essence to support overall skin barrier during the recovery window. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
Why Diastasis Recti Happens
The rectus abdominis is a paired muscle. The left and right halves run vertically from the lower ribs to the pubic bone, separated at the midline by a strip of dense connective tissue called the linea alba. This connective tissue is what holds the two halves of the muscle together and gives the abdominal wall its midline integrity. During pregnancy, the expanding uterus pushes outward against this connective tissue, stretching it laterally over many months. At full term, the linea alba can be stretched to 5 cm or more in width at the widest point, which is typically just above the navel.
After delivery, the connective tissue contracts again — but not always all the way. The factors that affect post-delivery recovery of the linea alba include: the number of pregnancies (each subsequent pregnancy is more likely to leave residual separation), the weight gained during pregnancy (more weight, more stretching), the position and size of the baby (large babies, twins, or babies in unusual positions stretch the linea alba more), maternal age (older mothers recover connective tissue less efficiently), pre-pregnancy core strength (stronger abdominal walls hold up better), and genetic connective tissue strength (varies by individual).
Diastasis recti is occasionally caused by significant weight fluctuation in non-postpartum patients, by repeated heavy lifting with poor form, or by chronic abdominal distension (some chronic medical conditions). But the dominant cause in the foreign patients arriving at Seoul clinics is postpartum.
The Self-Diagnostic Test at Home
This is the most-shared section in foreign mother forums because most patients have never been shown how to check for diastasis themselves. The test takes 30 seconds and gives a reasonably accurate measurement at home before any clinical visit.
Step 1. Lie flat on your back on a firm surface (the floor with a yoga mat works well). Bend your knees so your feet are flat on the floor. Relax your abdomen completely.
Step 2. Place one hand behind your head — palm under the back of your skull, fingers supporting your neck.
Step 3. Slightly lift your head and shoulders off the floor — just enough that your shoulder blades come up by an inch or two. Do not do a full sit-up. The point is to engage your abdominal muscles enough that you can feel them, but not so much that the abdominal wall pushes outward forcefully.
Step 4. With the fingers of your other hand pressed vertically into the midline of your abdomen — fingers pointing toward your head, knuckles flat against your belly — palpate the midline at three positions: about 5 cm above your navel, at the navel itself, and about 5 cm below your navel.
Step 5. At each position, feel for whether the abdominal wall is firm and continuous (no gap, your fingers don’t sink in), or whether there is a soft gap that your fingers can sink into. If there is a gap, count how many of your fingers fit side-by-side into it.
Under 1 finger-width is normal and does not need surgical repair. 1 to 2 finger-widths is a mild diastasis; many patients with this degree of separation can close it further with targeted physical therapy (specifically transverse abdominis activation exercises like dead bugs, bird dogs, and pelvic tilts — not crunches or sit-ups, which can worsen it). 2 to 3 finger-widths is a moderate diastasis that exercise often cannot fully close, especially if the patient is more than 12 months postpartum. 3 or more finger-widths is a significant diastasis that exercise alone is unlikely to resolve, and surgical plication is typically the only solution that returns the abdominal wall to its pre-pregnancy state.
Additional signs of significant diastasis: a visible vertical doming or bulge along the midline when the patient sits up from flat, a “coning” appearance during planks or core engagement, lower back pain that worsens with core exercises, and a soft pouch or pooch that persists despite weight loss to pre-pregnancy levels.
Why Exercise Alone Often Doesn’t Close a Significant Diastasis
This is the conversation foreign patients have already had with their physical therapist or postpartum exercise instructor, and they often arrive at the Seoul consultation skeptical. They have been doing the recommended exercises for 12 to 18 months. The gap has narrowed somewhat, perhaps from 3 fingers to 2. But it has not closed.
The reason is that significant separation of the linea alba is a connective tissue problem, not a muscle problem. The transverse abdominis activation exercises can strengthen the deep core musculature and bring the rectus muscles closer together by improving the resting muscle tone. But the linea alba itself — the stretched-out connective tissue between the muscle halves — does not contract significantly from exercise. Once it has been stretched beyond a certain point, it stays stretched. Physical therapy can take a 3-finger gap to a 2-finger gap by improving muscle activation, but it cannot take a 2-finger gap to zero because that requires the connective tissue itself to shrink, which it does not do.
This is why surgical plication is the only definitive solution for significant residual diastasis. The plication sutures bring the two muscle halves directly back to the midline and hold them there while scar tissue forms to reinforce the new closure. The result is a firm abdominal wall that no longer separates, regardless of whether the patient continues with core exercises post-operatively.
What Functional Improvements Patients Notice After Diastasis Repair
Foreign mothers consistently report that the functional improvements after diastasis repair surprise them. They booked the procedure for cosmetic reasons — to flatten the postpartum belly — and discovered post-operatively that their core function improved as well.
Common reports: reduced lower back pain (the lumbar spine no longer compensates for a weak anterior core), more efficient sit-ups and forward-bend mechanics (the abdominal wall now functions as a single unit), improved posture (the pelvic tilt and lumbar curve correct as the anterior core becomes capable of holding tension again), and easier return-to-running mechanics (the diaphragm and pelvic floor function more coordinatedly when the rectus is no longer separated). Some patients also report improvement in urinary stress incontinence — the pelvic floor and the abdominal wall function as a coordinated system, and reinforcing one improves the other.
None of these functional improvements are guaranteed for every patient, and they are not the primary reason the procedure is performed. But the patients who arrive prepared for a cosmetic result often leave with a better-functioning core as well, and Korean surgeons mention this explicitly during consultation as part of setting realistic expectations.
Section 4 — Recovery Timeline Week by Week for Postpartum Patients
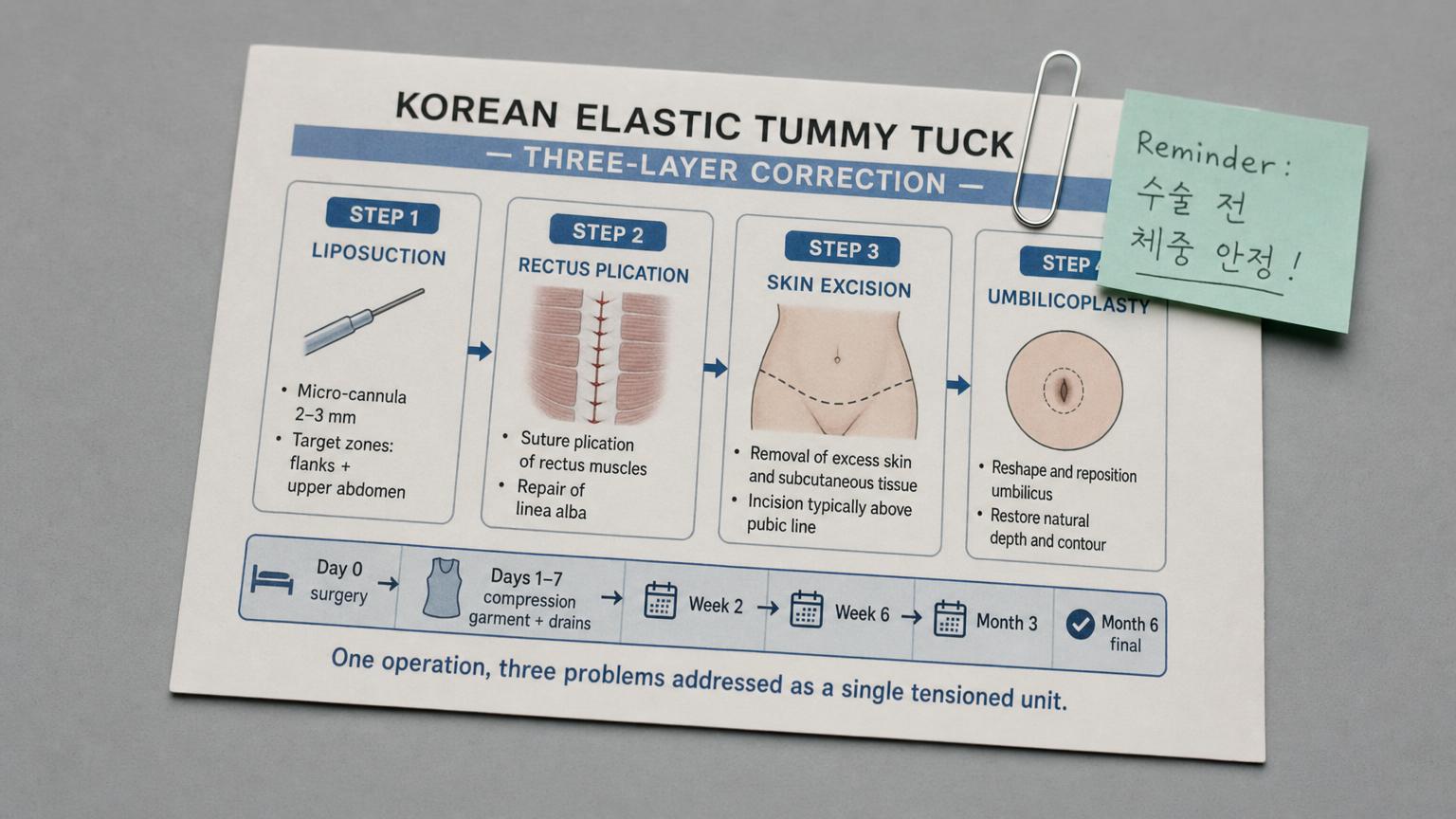
The Korean elastic tummy tuck is a more substantial procedure than standalone liposuction, and the recovery timeline reflects this. Foreign patients who try to compress the trip into the same 7-to-10 day window they would use for liposuction routinely run into trouble. The minimum trip length for a tummy tuck procedure in Seoul is 14 days; the preferred trip length is 21 days. Patients with childcare responsibilities at home often find this difficult to arrange — and that scheduling difficulty is one of the most important practical considerations the patient needs to plan around before booking.
Day 0 — Surgery Day
Anesthesia for the elastic tummy tuck is intravenous sedation supplemented by local infiltration of tumescent solution at the surgical zones, or general anesthesia for larger or more complex cases. The choice depends on the surgical plan, the patient’s history, and the surgeon’s preference. The operation typically takes 3 to 5 hours from incision to closure, depending on the volume of liposuction, the length of the diastasis to be repaired, and the amount of skin to be excised.
Immediately after surgery, the patient is dressed in a high-compression abdominal garment in the operating room, before the patient is fully awake. The garment stays on continuously from this moment. Drainage tubes are placed under the skin flap to collect tumescent fluid and serous discharge that accumulates in the first 48 to 72 hours — these are removed at the first or second post-operative follow-up depending on output volume. Most patients spend the first night in the clinic or an attached recovery facility under nursing observation; the next morning they are transferred to a hotel near the clinic.
Days 1 to 3 — Peak Swelling and Drainage
The first three days are the most uncomfortable phase of the recovery. The patient walks short distances (10 to 20 meters at a time, multiple times per day) to support circulation and reduce the risk of deep vein thrombosis, but otherwise rests in a slightly flexed position — typically reclining with knees bent — to keep tension off the abdominal closure. Sitting up flat is uncomfortable; standing fully upright is uncomfortable. The flexed posture is normal and resolves over the following two weeks.
Drainage from the small drain tubes is highest in the first 48 hours, then tapers. The patient or hotel staff records drainage volume morning and evening and reports it at the first follow-up visit. Pain is managed with oral analgesics; most patients do not need stronger medication beyond the first 48 hours. The compression garment stays on continuously except for very brief wipe-downs.
Day 7 — First Major Follow-Up
The patient returns to the clinic for the first major post-operative evaluation. The surgeon inspects the incision line, removes the drainage tubes if drainage has decreased sufficiently, and removes any superficial sutures or staples that were placed for skin closure. The compression garment fit is reviewed; if swelling has shifted the garment fit, an adjustment or replacement is provided. The patient is cleared to shower normally from this point if the incision is healing well.
This is also when many patients first see the surgical result without the compression garment in place. The contour at day 7 is still distorted by significant swelling and bruising. The patient is reminded explicitly not to evaluate the result at this stage — the final contour will not be visible for at least 6 weeks, and the result they came for is not what they are looking at now.
Day 14 — Final Suture Removal and Flight Clearance
The second major follow-up visit. Remaining sutures are removed, the incision line is inspected for healing progress, and the patient is evaluated for flight clearance. Korean clinics routinely refuse to clear patients for international flight before the day-14 visit. The risks of earlier flight include wound dehiscence under the pressure changes and prolonged sitting of long-haul flights, deep vein thrombosis from immobility, and seroma formation from fluid shifts. These are not abstract concerns — they are documented complications that occur at higher rates in patients who fly too early.
Patients cleared at day 14 are typically advised to wear the compression garment continuously during the flight, to walk the aisle every 60 to 90 minutes, to hydrate aggressively, and to wear graduated compression stockings to reduce deep vein thrombosis risk. Patients who plan to stay in Seoul through day 21 get an additional follow-up at day 21 before departure and tend to have smoother recovery from the journey home.
Weeks 3 to 6 — Compression Compliance Window
This is the window where most foreign patients fail compliance and end up with worse final contour than they could have had. The compression garment requirement at this stage is 16 to 20 hours per day, gradually tapering toward 12 hours per day by week 6. The patient can shower normally and remove the garment for washing (clinics recommend having two garments to alternate). Light walking and gentle daily activity are unrestricted; lifting heavier than 5 kg, core exercises, and impact activities (running, jumping, weight training) are restricted until week 8 at minimum.
The patients who wear the compression garment consistently through this window see smoother contour at week 6 and better-defined waistline at month 3 than the patients who decided after week 2 that they had “healed enough” to skip it. This is the single most important behavior that distinguishes the best outcomes from the mediocre ones. Korean clinics emphasize it heavily during pre-operative consent and at every follow-up visit. The garment is not a comfort item — it is shaping the final result by encouraging the skin envelope to retract evenly onto the new underlying contour and by reducing the risk of seroma in the dead space created by the skin elevation.
Week 6 to Week 8 — Activity Resumption
At 6 weeks, most patients can discontinue compression garment use for most of the day (some surgeons extend the schedule to 8 weeks for larger cases or for patients with significant skin laxity). Walking and gentle daily activity have been unrestricted since week 3, but more vigorous activity gradually resumes: light cardio at week 6, more strenuous cardio at week 7, lifting heavier than 5 kg at week 8, and impact activities (running, jumping, weight training) at week 8 to 10 depending on healing progress and surgeon clearance.
Core-targeted exercises — planks, sit-ups, crunches — should be reintroduced cautiously and not before week 10. The diastasis repair sutures are still consolidating their scar tissue reinforcement during the first 10 weeks, and aggressive core loading before then can stress the repair. Working with a physical therapist familiar with post-tummy-tuck recovery is helpful for guiding the return to core training.
Month 3 — Settled Contour
By the 3-month mark, the abdominal contour has fully settled. Residual swelling has resolved. The compression garment is no longer required. The patient is wearing normal clothing and the result is visible. This is the photograph the Korean clinic will reference when evaluating the result. Patients describe themselves as “having my pre-pregnancy stomach back, but better” or “looking like a slimmer version of myself with a flat belly that holds tension.” The change is dramatic compared to pre-operative baseline but the patient does not look like a different person — the result is consistent with the patient’s natural anatomy as it was before pregnancy.
Month 6 to Month 12 — Scar Maturation and Final Result
The contour does not change significantly after month 3, but the scars continue to mature. The horizontal bikini-line scar and the periumbilical scar (around the new belly button opening) are red and visible for the first 6 to 9 months, then gradually fade to fine pale lines by 12 to 18 months. Korean clinics provide scar care guidance from week 3 onward — silicone sheeting applied daily, sun protection (SPF 50+ on the scar line whenever the abdomen is exposed to sunlight, including through thin clothing), and gentle scar massage with a moisturizing cream.
Patients with darker skin tones may experience temporary post-inflammatory hyperpigmentation along the scar line that takes 9 to 15 months to fully resolve. Patients with a history of hypertrophic or keloid scarring elsewhere on the body should mention this at consultation; the surgeon may recommend additional scar management (steroid injection, silicone gel, or laser treatment at the 6-month mark) to optimize scar appearance.
Section 5 — Cost, Verification, and Coordinating With Other Korean Procedures
The Korean elastic tummy tuck is competitively priced relative to US, Australian, and UK abdominoplasty, primarily because Korean clinics integrate the liposuction component into the same operative session at no significant cost premium. The Korean price advantage is most pronounced for combined-procedure cases where the patient would otherwise be paying for tummy tuck and liposuction as separately scheduled procedures.
Cost Comparison Table
| Region | Procedure | Cost Range |
|---|---|---|
| Korea (Seoul) — Mini tummy tuck | Lower abdomen only, no full diastasis repair | KRW 6,000,000–9,000,000 (USD 4,500–6,700) |
| Korea (Seoul) — Full elastic tummy tuck | Full diastasis repair, skin excision, neo-umbilicoplasty, integrated lipo | KRW 9,000,000–16,000,000 (USD 6,700–11,900) |
| Korea (Seoul) — Elastic tummy tuck + breast augmentation (mommy makeover) | Combined operative session | KRW 16,000,000–24,000,000 (USD 11,900–17,800) |
| USA — Full abdominoplasty | Often without integrated lipo | USD 12,000–22,000 (lipo billed separately at USD 4,000–8,000) |
| Australia — Full abdominoplasty | Often without integrated lipo | AUD 18,000–32,000 (lipo billed separately at AUD 6,000–12,000) |
| UK / EU — Full abdominoplasty | Available in cosmetic surgery clinics | GBP 8,500–17,000 (lipo billed separately at GBP 3,500–6,500) |
The Korean pricing typically includes the surgeon fee, operating room and anesthesia, the first high-compression garment, drainage tubes and incision care supplies, and follow-up visits through the 6-week mark. Patients who need a second garment (often the case at the week 3 to week 4 wash schedule) pay separately. International patients should also budget for hotel accommodation for 14 to 21 days minimum, international flights, possible companion travel (many postpartum patients bring a partner or family member to assist with the first week of recovery, which is the most difficult period), and possible revision visits if a second targeted contouring session is needed at the 6-month mark.
Coordinating With Other Korean Body Procedures
The elastic tummy tuck is rarely the only procedure a foreign mother is considering on a Korea trip, and the Korean clinic protocol is helpful at coordinating multiple procedures within the same recovery window.
- Combined with breast augmentation or breast lift (the classic “mommy makeover”). The most common combined-procedure pattern for postpartum patients. Both procedures are performed in the same operative session, which extends operative time to 5 to 7 hours total but consolidates the recovery into one timeline. The compression garment requirement for the abdomen overlaps with the surgical bra requirement for the chest. Total trip length is 14 to 21 days, the same as for the tummy tuck alone. The Link Plastic Surgery breast surgery page describes the integration in more detail. Korean clinics will agree to this combination if total operative time stays under approximately 7 hours and the patient’s medical clearance supports it.
- Combined with additional liposuction zones. If the patient has body contouring needs beyond the abdominal zones already included in the elastic procedure — for example, the outer thighs (saddlebags), the inner thighs, or the upper arms — these can sometimes be added to the same operative session. The deciding factors are total operative time (under 7 hours total), total aspirate volume (under 4,000 ml), and the patient’s anesthesia tolerance. The Link PS liposuction page describes the per-zone protocol. Patients combining substantial extra liposuction with the tummy tuck typically extend their trip to 21 days for added recovery margin.
- Combined with facial fat grafting. Patients who want facial fat grafting can sometimes have the donor fat harvested from the same liposuction performed for the tummy tuck — the lower abdomen or inner thigh is a typical donor site, and only 50 to 100 ml of fat is needed for facial grafting. This is treated as a courtesy aspiration rather than a separate procedure and does not significantly extend operative time. The fat grafting itself is performed at the end of the tummy tuck session, with care to keep the patient’s overall operative time within safe limits.
- Combined with skin tightening adjuncts. Patients with significant skin laxity that may not respond fully to the surgical skin excision — typically older patients (over 45) or patients who lost substantial weight before the procedure — sometimes have radiofrequency skin tightening or other adjunct procedures scheduled 3 to 6 months after the primary tummy tuck. These are not performed in the same operative session.
Five Questions to Ask Any Tummy Tuck Clinic in Korea
- Do you perform diastasis recti repair as a standard part of the procedure, or only on selected patients? The right answer is that diastasis repair is included as a standard part of any full tummy tuck on a postpartum patient with significant separation. A clinic that treats diastasis repair as an optional add-on is offering a less structured procedure than the Korean standard supports for postpartum bodies.
- Is liposuction integrated into the same operative session, or scheduled separately? The right answer is integrated. The Korean elastic version specifically addresses the flank and upper abdomen contour in the same operation so that the post-operative contour is continuous. A clinic that schedules the liposuction separately is offering a less coordinated procedure and the foreign patient may end up paying for two separate trips.
- Do you preserve and reposition the original belly button, or construct a new one? The right answer is preserve and reposition (neo-umbilicoplasty). A constructed belly button typically looks surgical with visible scarring around the opening; the Korean technique of preserving the original gives a more natural appearance at 6 months.
- What is the earliest day you would clear me for international flight home? The right answer is day 14 at the earliest, with day 21 preferred. A clinic that says “you can fly home after a week” is overlooking the documented risks of early flight (wound dehiscence, deep vein thrombosis, seroma) and is taking on more post-operative risk than the Korean standard supports.
- What is your protocol if I develop a seroma or wound healing issue after I return home? The right answer is a defined remote follow-up protocol — photo-based check-ins at scheduled intervals, a named contact for urgent questions, and a clear plan for what counts as a normal-recovery concern versus what counts as a “see a local doctor immediately” concern. A clinic without a defined remote follow-up protocol is one to avoid for international patients.
Frequently Asked Questions
Is the Korean elastic tummy tuck just a different name for abdominoplasty?
Yes and no. The core surgical procedure is abdominoplasty — skin excision, rectus plication, neo-umbilicoplasty. What “elastic” refers to in the Korean context is that liposuction sculpting is integrated into the same operative session, so the abdominal wall is rebuilt as a single tensioned unit rather than three separate fixes done in sequence at different visits. The result is more continuous contour at the flanks and upper abdomen than what a standalone abdominoplasty without integrated liposuction can deliver.
How do I know if I actually have diastasis recti and not just stubborn belly fat?
Lie flat on your back with knees bent and feet on the floor. Place one hand behind your head and lift your head and shoulders slightly off the floor — just enough to feel the abdominal muscles engage. With the fingers of your other hand pressed vertically into the midline above and below your belly button, you should feel either a firm muscle wall or a soft gap. If you feel a gap wider than 2 fingers (about 2 cm), you have diastasis recti. If the gap is 3 or more fingers wide, or if you feel a doming or bulge along the midline when you engage your core, the diastasis is significant enough that exercise alone is unlikely to close it. Liposuction will not fix this — only surgical plication will.
Can I just do liposuction and skip the tummy tuck if I had a baby 2 years ago?
Only if the diastasis recti is mild (under 2 finger-widths) and the skin envelope still has good elasticity. Most postpartum patients arriving for consultation 18 months to 5 years postpartum have at least one of these three problems remaining: a residual diastasis gap, a stretched skin envelope that does not retract, or a deformed belly button. Liposuction addresses none of these. The patient who is best served by liposuction alone is the postpartum patient with minimal diastasis, good skin tone, and a localized fat pocket — typically someone under 35 years old whose body recovered well from pregnancy and who has a specific contour issue rather than a structural one.
How long do I need to stay in Korea for a tummy tuck procedure?
Minimum 14 days, with 21 days preferred. Day 0 is surgery, days 1 to 3 are peak swelling and drainage, day 7 is the first major follow-up visit and partial suture removal, day 14 is the second follow-up and final suture removal, and days 14 to 21 are the safe window for international flight clearance. Patients who try to fly home before day 14 risk wound dehiscence (the skin closure opening up) under the pressure changes and prolonged sitting of long-haul flights. Korean clinics routinely refuse to clear patients for flight before the day-14 follow-up. Plan the trip around this — not the other way around.
Will the new belly button look natural?
The Korean approach preserves your original belly button (the stalk that connects it to the abdominal wall) and re-positions it through a new opening cut in the tightened skin. This is technically called neo-umbilicoplasty. Because it is your original belly button, the appearance after healing is typically natural — a deeper vertical or hooded shape similar to what you had before pregnancy stretched it. Foreign patients sometimes assume the belly button is replaced or constructed from scratch, which would look obviously surgical; the Korean technique is to keep the original and reposition it, which is why it looks like a normal belly button at 6 months.
What is the difference between a mini, full, and elastic tummy tuck?
A mini tummy tuck addresses only the area below the belly button with a smaller horizontal incision; it does not include diastasis repair above the navel or belly button repositioning. This is rarely the correct procedure for postpartum patients because postpartum diastasis usually extends above the navel as well. A full tummy tuck addresses the full vertical span from xiphoid (lower ribs) to pubis, includes diastasis repair across the full length, and includes belly button repositioning. The Link PS elastic version emphasizes integrated liposuction sculpting in the same operative session, so the flanks and upper abdomen are contoured at the same time as the abdominal wall is tightened — without this, the lateral waistline can look mismatched relative to the newly flat abdomen.
Can I get pregnant again after a tummy tuck?
Yes, but it is medically recommended to wait until you have completed your family. Pregnancy after a tummy tuck stretches the abdominal wall again, can partially undo the diastasis repair (the sutured midline can be re-separated by the pressure of a growing uterus), and stretches the skin envelope. The cosmetic result will not be the same after a second pregnancy. The Korean clinical practice is to ask postpartum patients at consultation whether they consider their family complete; patients who are still planning more children are typically advised to wait, and to address the postpartum body with non-surgical options (skin tightening, conservative liposuction) in the interim.
What is the scar like, and where is it placed?
The main incision is horizontal, placed low on the abdomen along what Korean surgeons refer to as the bikini line — low enough to be covered by underwear, swimwear bottoms, and most low-rise clothing. The length of the scar varies with how much skin needs to be removed, but typically extends from one anterior superior iliac spine (the bony prominence at each hip) to the other. There is also a small periumbilical scar around the new belly button opening. Both scars are red and visible for the first 6 to 9 months, then gradually fade to fine pale lines by 12 to 18 months. Korean clinics emphasize scar care from week 3 onward — silicone sheeting, sun protection, and gentle massage — because scar maturation is one of the most important outcomes a postpartum patient cares about long-term.
I had a C-section. Does that change the procedure?
Often it simplifies the cosmetic result rather than complicating it. The Korean surgeon will typically incorporate the existing C-section scar into the new abdominoplasty incision rather than creating a separate scar — this means you end up with one well-placed horizontal scar instead of two. Additionally, the soft pouch of skin and fat that often sits above an old C-section scar (sometimes called a “C-section shelf” or “fupa”) is addressed by the same skin excision that closes the diastasis repair. Patients with C-section history are some of the most satisfied postpartum tummy tuck patients because the procedure simultaneously cleans up the old surgical scar appearance and resolves the persistent shelf above it.
How does Korean cost compare to US or Australian tummy tuck pricing?
Korean elastic tummy tuck pricing is typically 30 to 50 percent less than equivalent US or Australian abdominoplasty pricing, with substantially better integration of liposuction in the same operative session. A full elastic tummy tuck in Seoul ranges from KRW 9 to 16 million (USD 6,700 to 11,900), inclusive of surgeon fee, operating room, anesthesia, first compression garment, and follow-up visits through the 6-week mark. The same procedure in the United States ranges from USD 12,000 to 22,000 typically, often with liposuction billed separately. In Australia the range is AUD 18,000 to 32,000. The Korean pricing typically does not include hotel accommodation (14 to 21 days), international flights, or possible revision visits if a second targeted contouring session is needed at the 6-month mark.
Closing
The Korean elastic tummy tuck for postpartum patients is built around a layered correction that foreign mothers do not arrive expecting. The procedure addresses three distinct problems — subcutaneous fat, separated rectus muscles, and a stretched skin envelope with a deformed belly button — through three coordinated surgical layers performed in one operative session. Liposuction alone solves none of these structurally. A tummy tuck without integrated liposuction leaves the lateral contour mismatched. A mini tummy tuck addresses only the lower portion and leaves postpartum diastasis above the navel unrepaired. The full elastic version is the procedure that delivers a coherent post-operative result for the postpartum body — flat midline, continuous flank-to-flank contour, a naturally positioned original belly button, and a scar that fades to a fine line under low-rise clothing.
Foreign mothers who arrive in Seoul expecting strong liposuction to do the job leave the consultation surprised by how much structural work was actually hidden inside their postpartum belly. The patients who do best are the ones who arrive willing to have the layered conversation — who understand that the bulge is not just fat, that exercise has done what exercise can do, and that the structural separation of the rectus muscles needs a structural answer. The Korean protocol fluency, integrated operative session, and 14-to-21 day recovery infrastructure that has developed around postpartum surgical contouring in Seoul over the last two decades is what makes Korea a practical destination for the procedure. Clinics built around this protocol — including the elastic tummy tuck program detailed on Link Plastic Surgery’s official website — will set those expectations honestly during consultation, will perform the integrated procedure as a single coordinated operation, and will clear the international patient for the journey home only when the healing supports it. That sequence, more than any individual technique, is what makes the Korean elastic tummy tuck the procedure that postpartum foreign mothers eventually find themselves searching for, once they understand what they actually need.