Korean Epicanthoplasty (Inner Corner): What Foreign Patients Should Know Before Adding It

Foreign patients arriving in Seoul for double eyelid surgery often discover, during the consultation, that the surgeon is recommending an additional procedure they had not researched. That procedure is epicanthoplasty, the structural release of the Mongolian epicanthal fold that covers the inner corner of the eye. The recommendation is not upsell. In approximately 60 to 75 percent of Korean double eyelid consultations the surgeon assesses whether the fold will compete with the new crease and recommends epicanthoplasty when an unaddressed fold would pull the inner end of the new line downward or shorten the crease into a half-formed appearance. Foreign patients who treat this recommendation as “the clinic trying to sell more surgery” frequently regret declining it at the 6 to 9 month mark when the new crease has settled but the inner corner remains covered. Foreign patients who accept the recommendation without understanding what it actually does sometimes overshoot in the other direction and ask for an aggressive release that delivers an unnaturally wide inner-eye exposure. The honest answer sits between the two extremes, and it depends on anatomy that the surgeon can read but the patient cannot read on their own face. Link Plastic Surgery in Seoul is one of the clinics that runs the four-technique decision framework during consultation rather than applying a single standardized technique to every patient, which is the practice pattern this guide treats as the verification standard.
The technical content matters because epicanthoplasty has two failure modes that look opposite but share the same root cause. The first failure mode is over-correction, where the lacrimal caruncle is exposed too aggressively and the inner corner takes on an unnaturally rounded or “Western” appearance that does not match the rest of the Asian eye shape. The second failure mode is visible scar, where the incision was placed off the natural shadow line and remains apparent at 6+ months. Both failures share a common root: the technique was selected by the surgeon’s preference or the clinic’s standard protocol rather than by the patient’s specific fold anatomy. The four standard Korean techniques exist precisely because no single approach fits every fold, and the surgeon who can explain why your fold calls for Technique A rather than Technique B is the surgeon who is treating epicanthoplasty as a structural decision. The surgeon who applies the same technique to every patient is the surgeon whose results regress to the mean — some patients look great, some look over-corrected, some have visible scars — without a coherent anatomical reason for the distribution.
Section 1: What Epicanthoplasty Actually Is (And What It Is NOT)
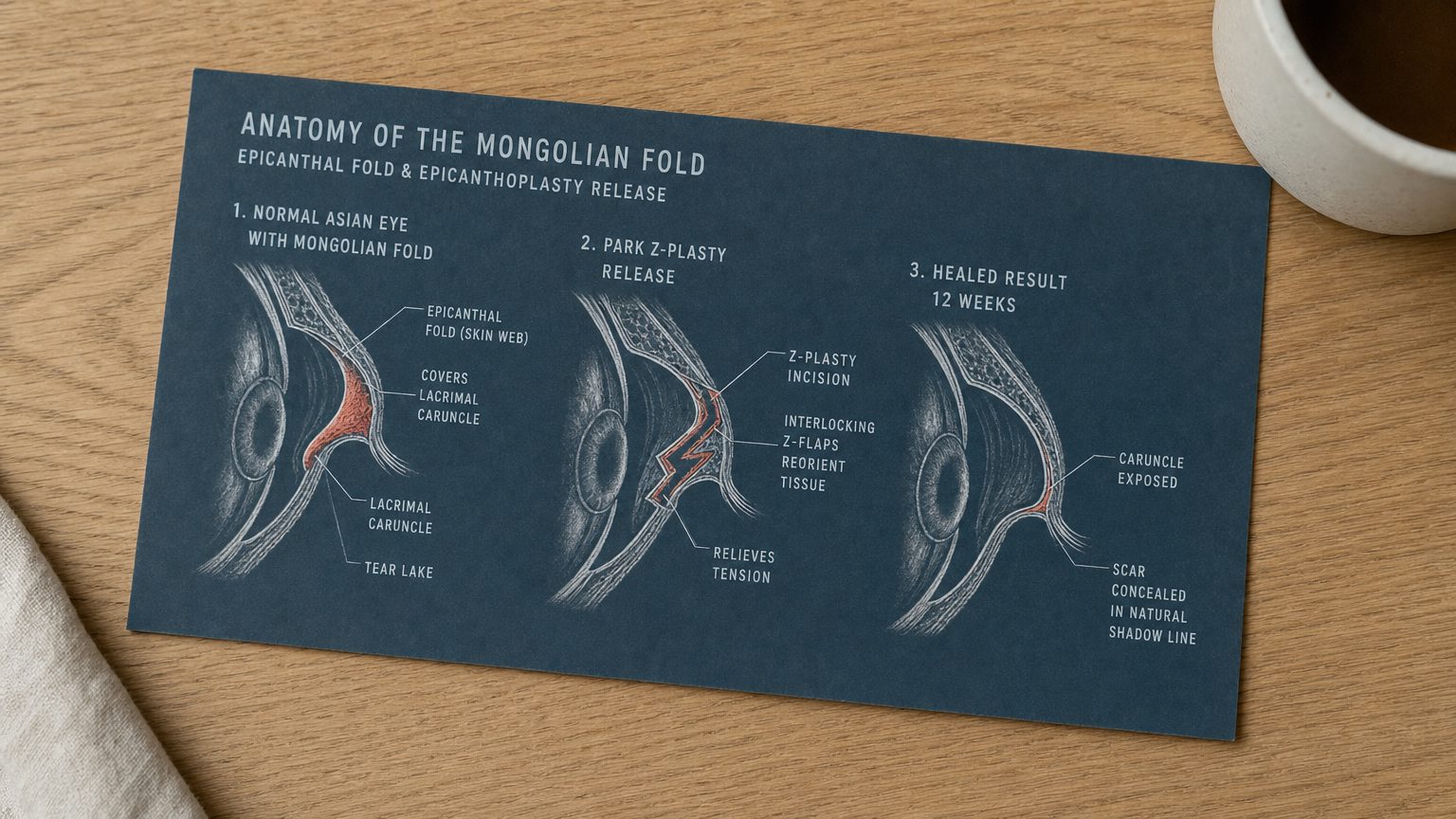
The Mongolian fold, formally called the epicanthal fold or epicanthus, is a small web of skin that originates from the upper eyelid and curves down to attach near the lacrimal caruncle, the small pink mound at the inner corner of the eye where the tear duct opens. The fold is present in approximately 50 to 90 percent of patients of Korean, Chinese, Japanese, and other East Asian ancestry, with prevalence varying by population and individual genetics. Less than 10 percent of Caucasian patients have a comparable fold, which is why Western plastic surgery does not have a standard epicanthoplasty procedure in its primary catalog. The fold is not a pathology — it is a normal anatomical variant in East Asian eye structure — but for patients who also pursue double eyelid surgery, the fold can interfere with the new crease in ways that produce aesthetically suboptimal results.
The procedure called epicanthoplasty releases the fold by making a small carefully designed incision that allows the skin web to be repositioned, exposing the lacrimal caruncle and widening the visible inner intercanthal distance. The result is not a larger eye dimension. The orbital bone, the lid margins, and the actual eye opening are unchanged. What changes is the proportion of pink caruncle visible relative to skin coverage, and the angle at which the inner corner meets the rest of the eye shape. The change is subtle on still photos and more visible on dynamic expression and in person, because the inner corner contributes substantially to overall eye-shape perception in motion. The clinic-level technical breakdown is published in Link Plastic Surgery’s Korean epicanthoplasty procedure page, which is the primary source for the four-technique decision framework discussed below.
Four Common Foreign Patient Misconceptions
Misconception 1: Epicanthoplasty is just making the eyes bigger or wider. The procedure does not change the orbital dimensions or the actual eye opening. It exposes the lacrimal caruncle that was previously covered by the fold. The perceived widening is the visible inner intercanthal distance, not an actual increase in eye size. Patients who arrive at consultation asking for “bigger eyes” are often asking for a combination of double eyelid surgery and epicanthoplasty, sometimes with a lateral canthal procedure, and the surgeon’s job is to clarify what each component actually changes.
Misconception 2: Korean epicanthoplasty is the same as Western inner-corner lift. Western inner-corner procedures, including various forms of medial canthoplasty and medial canthal repair, target anatomy that is structurally different from the Mongolian fold. A Western canthoplasty performed on an Asian patient with a Mongolian fold either does not address the fold at all (if the surgeon treats the procedure as a Western canthoplasty) or addresses it incorrectly (if the surgeon applies Western technique to anatomy it was not designed for). Korean surgeons performing epicanthoplasty use Korean-developed techniques specifically calibrated to Mongolian fold anatomy. A surgeon outside of Korea, or in Korea but trained primarily in Western technique, may not be the right operator for this specific procedure.
Misconception 3: Epicanthoplasty is a standalone aesthetic widening that can be done in isolation as a “starter” procedure. In a meaningful subset of cases, epicanthoplasty is performed alone, particularly for patients who already have a natural or surgical double eyelid but whose inner corner remains covered. Standalone cases account for approximately 15 to 25 percent of Korean epicanthoplasty volume. The remaining 75 to 85 percent are combined with double eyelid surgery, because the fold and the crease interact and the structural release allows the new crease to flow naturally into the inner corner. Patients who think of epicanthoplasty as a small “starter” procedure to test the surgeon often discover that the fold and the existing crease (if any) are already in a stable relationship and that changing one component shifts the other in ways that were not anticipated.
Misconception 4: The result is permanent in the same way that bone surgery is permanent. The skin release itself is structurally permanent in the sense that the fold has been physically repositioned. However, scar maturation and tension dynamics continue to evolve for approximately 12 months after surgery. The appearance at week 4 is not the appearance at month 6 is not the appearance at month 12. Patients who evaluate their result at week 4 or week 8 frequently come to different conclusions than they reach at month 6 once full maturation has settled. The “is it permanent” question, properly asked, becomes “when does the final result actually appear” — and the answer is month 6 at earliest, month 12 with full confidence.
What Epicanthoplasty Actually Is, Structurally
The procedure is a controlled release of the epicanthal fold using one of four standard incision and repair patterns. The specific pattern is selected by the surgeon based on fold thickness, lacrimal caruncle position relative to the skin web, the angle at which the existing or planned double eyelid line will meet the inner corner, and skin tension dynamics in the surrounding area. The surgeon makes a small incision (the design of which varies by technique), releases the skin web from its anchoring points, and re-sutures the released skin so that the lacrimal caruncle is exposed and the surrounding skin sits in a natural relationship to the rest of the eye. The procedure typically takes 30 to 45 minutes per eye when performed as a standalone, and 60 to 90 minutes total when combined with double eyelid surgery as a single operation.
Why Korean Clinics Call It a Complement Rather Than a Procedure
The framing matters. A clinic that treats epicanthoplasty as a standalone aesthetic procedure tends to recommend it indiscriminately as a way to “make eyes bigger” for any patient who walks in asking for that. A clinic that treats epicanthoplasty as a complement to double eyelid surgery applies it selectively, based on whether the fold will compete with the new crease in the specific patient’s anatomy. The complement framing is the structurally honest one because in patients where the fold does not interfere with the existing or planned crease, epicanthoplasty adds risk (scar, recovery, over-correction potential) without commensurate benefit. The patients for whom epicanthoplasty is most clearly indicated are patients with thick folds that already shorten or distort the existing crease, or patients planning double eyelid surgery whose fold will pull the new crease downward at the inner end.
Readers landing on this guide first may also want to read our coverage of Korean double eyelid surgery for the foundation procedure that epicanthoplasty most commonly accompanies, and our guidance on inner-corner anatomy in the context of tear trough diagnostics for related anatomical decisions.
Section 2: The Four Korean Epicanthoplasty Techniques (Anatomical Decision, Not Patient Preference)
The four standard techniques are not interchangeable, and the choice is not preference-based. The surgeon selects the technique by reading the patient’s fold anatomy during consultation. A surgeon who applies the same technique to every patient regardless of anatomy is either treating epicanthoplasty as a standardized service or has a single technique they consider universally superior — neither of which produces the best result across a heterogeneous patient population.
Technique 1: Park Z-plasty (Modified)
The Park Z-plasty is the Korean standard for moderate folds and is the most commonly performed technique across the foreign patient population. The incision pattern consists of two interlocking Z-shaped incisions that release the skin tension in the fold and redirect the resulting scar along the natural shadow lines of the inner-eye contour. The technique works particularly well for folds of moderate thickness where the lacrimal caruncle sits in a position that allows the released skin to drape naturally over the new exposure. Recovery for sutures is approximately 7 to 10 days, with scar maturation reaching the barely-visible stage by week 12.
Patients for whom Park Z-plasty is the right technique typically have folds that cover the lacrimal caruncle but do not significantly distort the eye shape, and existing or planned double eyelid lines that meet the inner corner at a relatively obtuse angle. The technique provides moderate release with minimal over-correction risk, which is why it is the workhorse procedure for Korean epicanthoplasty practice.
Technique 2: Root Z-plasty
The root Z-plasty is a deeper release approach used for thick folds with significant skin redundancy where a more aggressive release is required to fully expose the lacrimal caruncle. The incision pattern is similar in geometry to the Park Z-plasty but extends deeper into the skin web at the root of the fold (the point where the fold attaches to the surrounding tissue). The deeper release allows more skin to be repositioned, which means the resulting exposure is more dramatic but the scar at the 3-month mark is also slightly more visible before fully maturing by month 9.
Many senior Seoul surgeons, including those at Link Plastic Surgery, prefer root Z-plasty for first-time patients with strong folds because the technique produces a more definitive correction that is less likely to require revision. The trade-off is the longer scar maturation window. Patients selecting between Park Z-plasty and root Z-plasty should ask the surgeon to explain why the recommended technique fits the patient’s specific fold and what the expected difference in scar appearance would be at the 3-month, 6-month, and 12-month marks.
Technique 3: V-W Plasty
The V-W plasty is a minimal-incision approach for thin folds with mild caruncle coverage, where a small precise release is sufficient to expose the inner corner. The incision pattern is shorter than either Z-plasty technique, recovery is the fastest of the four (sutures out at day 5 to 7, full healing by week 6 to 8), and the scar is the most subtle. The trade-off is that the release is limited and the technique is not suitable for patients who want or need significant inner-corner exposure.
Patients for whom V-W plasty is the right technique typically have folds that are present but not dominant, lacrimal caruncles that are partially visible already, and a goal of subtle refinement rather than significant inner-corner widening. The technique is sometimes selected for younger patients who want a minimal intervention or for patients who already have a natural double eyelid and want only the inner-corner refinement.
Technique 4: Skin Redraping (Modified Flap)
The modified skin redraping approach is the most technically complex of the four and is typically reserved for revision cases, congenitally asymmetric folds, or patients with unusual anatomy that does not fit cleanly into the Z-plasty or V-W categories. The technique uses local skin flaps to reposition tissue in a more individualized pattern, and the planning is more involved than for the standard techniques. Recovery is longer (sutures out at day 8 to 10, full healing by week 12 to 16) and scar maturation extends to month 12 to 14 in some cases.
Patients for whom skin redraping is indicated typically have a previous epicanthoplasty that produced suboptimal results and requires a revision approach, or congenital asymmetry where the two epicanthal folds are different enough that a single standardized technique cannot address both eyes coherently. The technique is in the operative repertoire of all senior Korean epicanthoplasty surgeons but is performed less frequently than the three primary techniques.
Why Technique Choice Is Anatomical, Not Preference-Based
The surgeon evaluates several specific anatomical factors when selecting the technique: fold thickness (thin folds favor V-W plasty, moderate folds favor Park Z-plasty, thick folds favor root Z-plasty), lacrimal caruncle position relative to the medial canthus (closer caruncles call for more conservative release to avoid over-exposure), distance to the medial canthus and inner intercanthal width (narrow intercanthal distance limits how much widening is anatomically appropriate, because excessive widening produces an unnatural close-set or “crossed” appearance), risk of tear duct exposure (the lacrimal puncta should remain protected by surrounding tissue and an over-aggressive release can leave the puncta visible in a way that is both aesthetically and functionally undesirable), and the angle of the existing or planned double eyelid line where it will meet the inner corner.
A patient cannot choose Park Z-plasty if their anatomy indicates root Z-plasty would produce a better result and prevent reverse-pulling tension on the new crease. A patient cannot choose V-W plasty if their fold is thick enough that minimal release will not adequately expose the caruncle. The technique is selected by reading the anatomy, not by patient preference for a faster recovery or a smaller scar. Surgeons who allow patients to choose the technique from a menu are typically not performing the structural assessment that the procedure actually requires.
Cross-Reference to Related Anatomical Decision-Making
Readers interested in how Korean surgeons make similar anatomical decisions across other eye procedures can review our coverage of Korean upper eyelid fat removal, which demonstrates the same anatomical-decision framework applied to a different structural component of the upper eyelid. The pattern is consistent: Korean eye surgery treats each component (epicanthal fold, levator function, ROOF fat, septum, orbicularis muscle) as an individually assessable structure, and the patient’s specific combination of these components dictates which procedures are recommended and which techniques are selected within those procedures.
Section 3: Why Korean Clinics Pair Epicanthoplasty With Double Eyelid Surgery (And When They Don’t)
The structural pairing logic between epicanthoplasty and double eyelid surgery is the single most important concept in Korean eye surgery for foreign patients to understand. Korean surgeons do not recommend epicanthoplasty as an upsell — they recommend it as a structural complement when the patient’s fold anatomy will interfere with the planned crease. Understanding why the interference happens, and why the interference produces a specific aesthetic problem, is the difference between a foreign patient who accepts or declines the recommendation thoughtfully and a foreign patient who makes the decision based on cost or fear.
Recommended for Your Recovery
Products commonly used before and after Korean epicanthoplasty inner corner — same items routinely recommended in the recovery instructions Seoul clinics hand out at discharge.
- Arnica Montana Tablets — begin 3 days before eyelid surgery to reduce periorbital bruising and swelling. Check price on Amazon
- Gel Eye Mask (Cold Compress) — reusable cold pack for the every-two-hour icing schedule on day 1 to day 3. Check price on Amazon
- Silicone Scar Sheets — apply from week 3 onward along the upper lid incision line if your procedure was incisional. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — lightweight Korean sunscreen to protect the healing scar and prevent post-inflammatory pigmentation. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
The Structural Pairing Logic Explained
When a double eyelid line is created surgically, the new crease meets the inner corner of the eye at a specific angle determined by the surgeon’s design and the patient’s anatomy. In patients without a significant Mongolian fold, the new crease can flow naturally into the inner corner because there is no competing fold pulling the inner end downward. In patients with a thick Mongolian fold, the fold acts as a downward tension vector at the inner corner. The new crease, anchored at its outer end by the levator mechanism and at its inner end by the surgically created suture line, gets pulled by the fold tension into a shortened or angled appearance.
The specific failure modes from an unaddressed fold include: the inner end of the new crease may angle downward in a way that does not match the rest of the crease line, the crease may appear to “disappear” or shorten at the inner end as the fold tension pulls the skin together, the eye may take on a “half-closed” appearance because the fold continues to cover what should now be visible double eyelid space, and the patient may report feeling that the surgery “did not give them the full result” because the crease they paid for is partially hidden by the fold.
An adjunctive epicanthoplasty performed at the same time as double eyelid surgery releases the fold tension so the new crease can flow naturally into the inner corner without being pulled. The two procedures together produce a coherent eye shape where the crease, the inner corner, and the surrounding tissue all sit in a stable structural relationship.
The Statistical Pattern in Korean Practice
The 60 to 75 percent recommendation rate in Korean double eyelid consultations is not a fixed clinic policy. It is the empirical rate at which fold anatomy actually interferes with the planned crease across the typical patient population. Foreign patients who hear “the surgeon recommends epicanthoplasty” can verify whether this is anatomical or commercial by asking the surgeon to explain specifically what about their fold and their planned crease angle is generating the recommendation. A surgeon who can answer with “your fold is approximately X mm thick, your planned crease will meet the inner corner at approximately Y degrees, the fold will pull the inner end downward by approximately Z mm without release” is treating it as an anatomical decision. A surgeon who answers with “most patients add this” or “it gives a more beautiful result” without anatomical reasoning is recommending it as a default service rather than as a structural assessment.
When Korean Surgeons Recommend Against Adding Epicanthoplasty
The 25 to 40 percent of cases where epicanthoplasty is NOT recommended are equally informative. Surgeons specifically advise against adding the procedure when:
- The fold is mild and caruncle exposure is already adequate. Patients whose folds cover only a small portion of the caruncle and whose planned crease will meet the inner corner at an obtuse angle often get sufficient inner-corner visibility without intervention. Adding epicanthoplasty in these cases produces marginal aesthetic gain at the cost of scar risk and recovery time.
- The inner intercanthal distance is already narrow (under 32 mm). Patients with naturally close-set eyes can develop an unnatural “crossed” or “doll-like” appearance if the inner corners are widened beyond what the underlying bone structure supports. Korean surgeons measure intercanthal distance during consultation and decline epicanthoplasty for patients whose anatomy will not tolerate the widening.
- The lacrimal caruncle is naturally prominent. Some patients have an above-average caruncle size that would appear visually conspicuous if fully exposed. Surgeons in this situation either decline epicanthoplasty or recommend a very conservative V-W plasty that exposes the caruncle minimally.
- The patient has a history of thin or sensitive scar healing. Patients with documented keloid tendency, dark or pigmented post-surgical scar patterns, or thin skin that demonstrates unusual scar visibility on previous surgeries are higher-risk candidates for visible epicanthoplasty scars. Surgeons may decline to recommend the procedure or recommend a more conservative technique with lower scar burden.
The Standalone Epicanthoplasty Case Profile
Approximately 15 to 25 percent of Korean epicanthoplasty consultations are for standalone procedures, where the patient is not undergoing primary double eyelid surgery at the same time. The two most common standalone case profiles are:
Patients with natural double eyelids whose inner corner remains covered. Some patients are born with a double eyelid line but also have a Mongolian fold that hides the inner corner. The natural crease is otherwise satisfactory, but the inner-corner coverage limits the perceived eye-shape harmony. Epicanthoplasty in these cases is purely the fold release without any change to the crease itself.
Patients who had double eyelid surgery elsewhere without epicanthoplasty and want to address the inner corner separately. Patients who underwent double eyelid surgery in another country or at a clinic that did not perform the anatomical assessment often arrive at Korean clinics 6 to 24 months later asking why their crease looks shortened or covered. The answer is typically that the fold was not addressed. A separately staged epicanthoplasty can be performed to release the fold and allow the existing crease to be more fully visible. The technique selection for these revision-context cases accounts for the existing crease position and the desired final relationship between the crease and the inner corner.
Standalone epicanthoplasty has shorter recovery than combined surgery (7 to 10 days for sutures, full social recovery in 2 weeks) and lower total cost (KRW 1,200,000 to 2,500,000 standalone versus KRW 3,500,000 to 6,000,000 combined). The procedure is also lower-risk because the surgeon is operating on a single structure rather than coordinating two interacting structures.
Reverse Epicanthoplasty
For patients who had over-aggressive epicanthoplasty elsewhere and want to soften the result, reverse epicanthoplasty exists as a revision procedure. The technique uses local skin flaps to rebuild a partial fold over the lacrimal caruncle, restoring a more natural inner-corner appearance for patients who feel their original procedure exposed too much caruncle or produced an unnaturally rounded inner corner. The reverse procedure is technically more demanding than the original epicanthoplasty because the surgeon is rebuilding rather than releasing, and is reserved for patients with clear over-correction. Most Korean surgeons performing reverse epicanthoplasty have several years of standard epicanthoplasty experience before adding the reverse procedure to their practice.
Section 4: Recovery, Scar Maturation, and the 12-Week Timeline

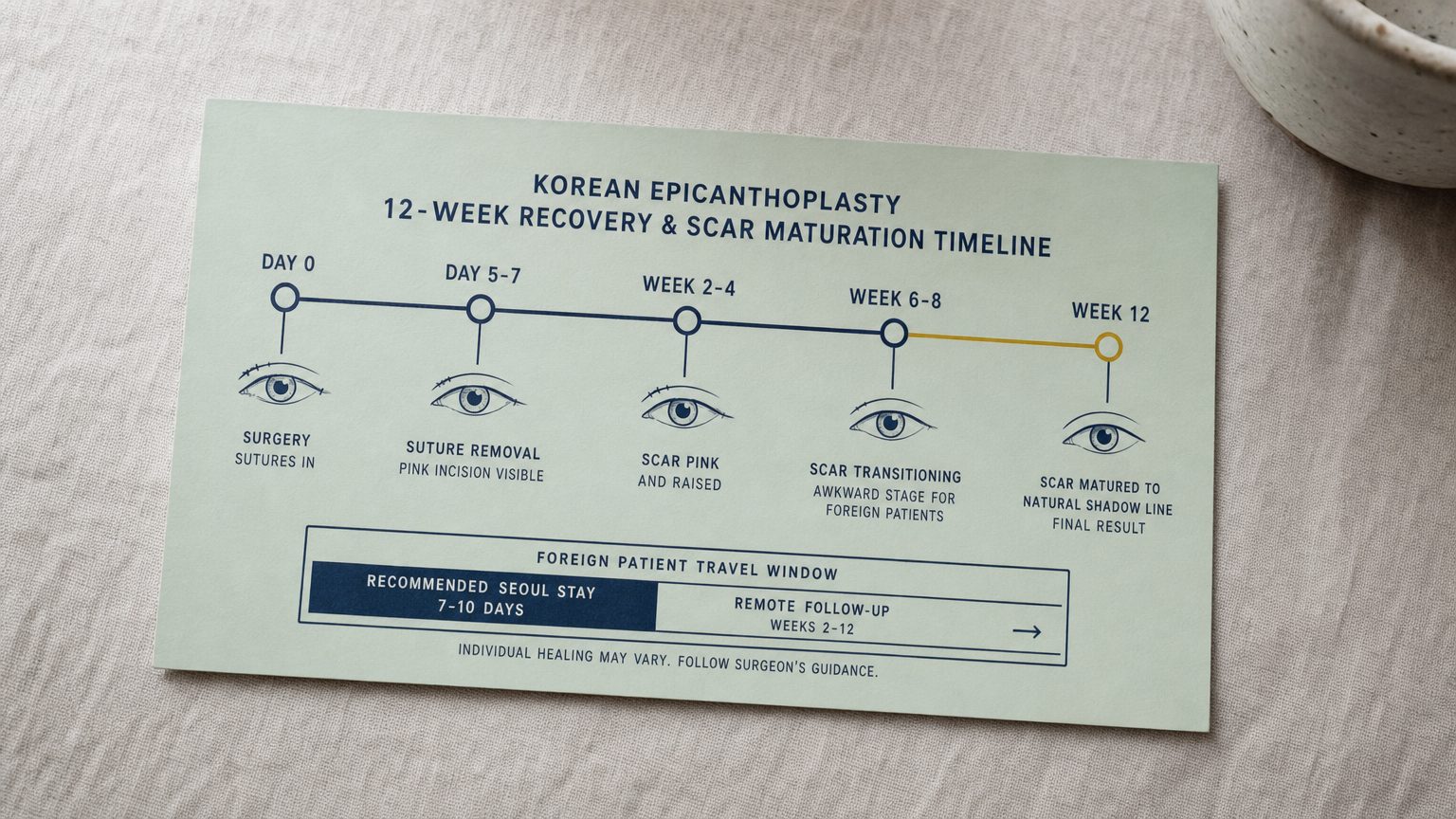
The 12-week timeline is the realistic window in which the procedure result actually appears. Foreign patients who evaluate their result at week 2, week 4, or even week 6 frequently come to different conclusions than they reach at week 12 once the scar has matured to its near-final appearance. Understanding the timeline week by week prevents the anxiety pattern where patients message the clinic at week 3 worried that the scar is “too visible” only to find at week 10 that the scar has settled into the natural shadow line as expected.
Day 0: Surgery
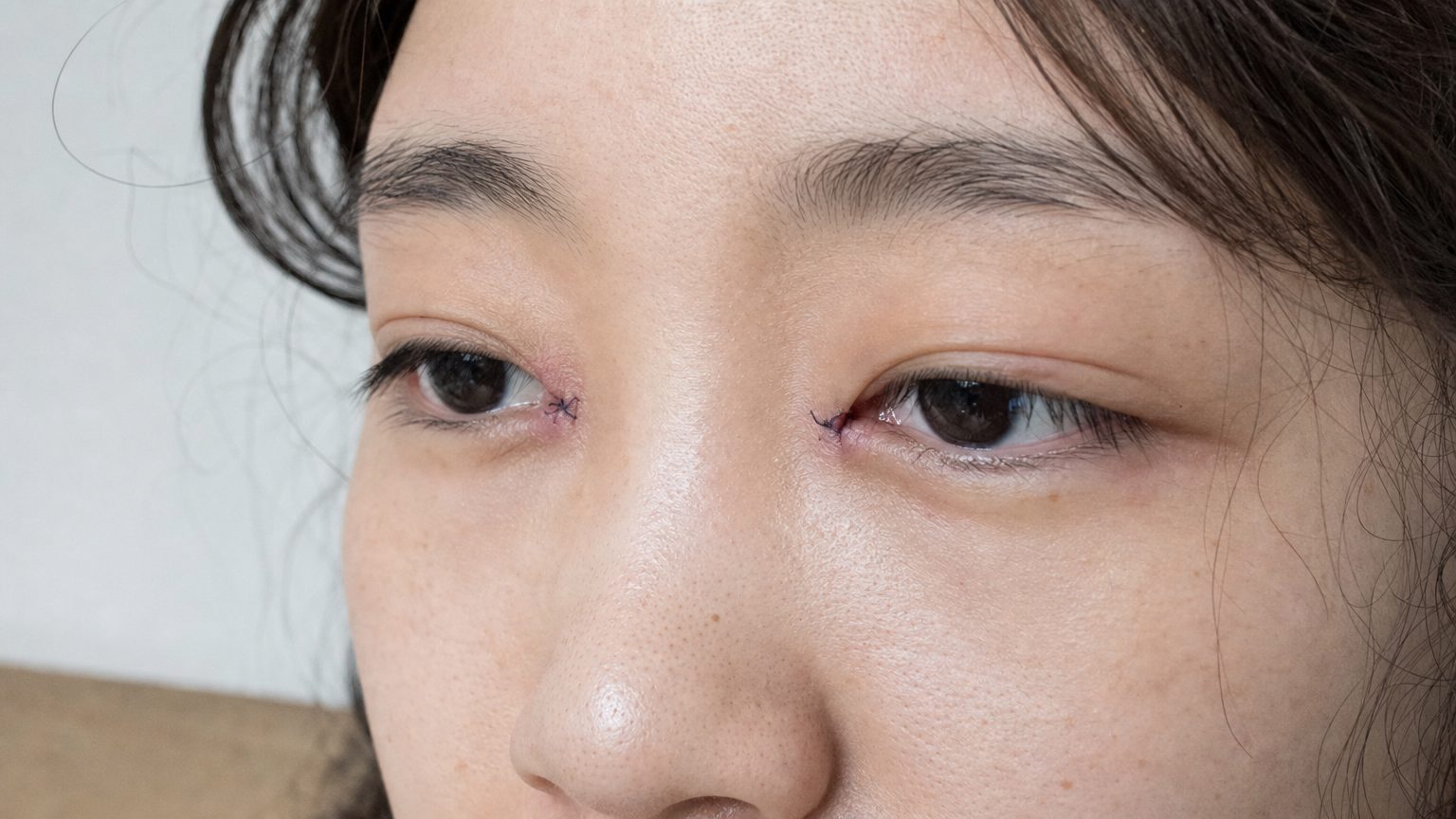
The surgery is performed under local anesthesia with mild oral sedation, or in some clinics under twilight sedation managed by the surgical team. The procedure takes 30 to 45 minutes per eye for standalone epicanthoplasty, 60 to 90 minutes for combined epicanthoplasty and double eyelid surgery. Patients walk out within 30 minutes of the end of surgery wearing protective sunglasses, with small surgical sutures visible at the inner corners. The immediate post-operative period involves mild discomfort that responds to standard oral analgesia.
Days 1 to 3: Initial Recovery
The first 72 hours show the most visible swelling and inflammation. Patients typically rest at the hotel or guesthouse, apply cold compresses (15 minutes on, 15 minutes off) for the first 48 hours, and avoid bending, lifting, or any activity that increases blood pressure in the head. Swelling peaks around day 2 to 3. Most patients have no significant bruising — epicanthoplasty rarely produces the yellow bruising pattern seen in lower-eye procedures because the surgical field is small and the vasculature in the area is less prominent. Patients can walk to nearby restaurants for soft food, but most prefer to have meals delivered to the room during this window.
Days 5 to 7: Suture Removal
Sutures are removed at day 5 to 7 depending on technique. The Park Z-plasty and V-W plasty typically allow earlier removal (day 5 to 6). The root Z-plasty and skin redraping typically require longer suture retention (day 7 to 9). The suture removal appointment is brief (15 to 20 minutes) and produces immediate improvement in the appearance of the inner corner because the suture marks disappear and the incision line is exposed for the first time. The incision at this stage is pink and slightly raised, which is normal and expected.
Week 2 to 4: The Pink and Raised Phase
The scar passes through its most visible phase between week 2 and week 4. The incision is pink to light red, slightly raised above the surrounding skin, and visible in close-up photographs. Patients sometimes panic during this window because they expected the scar to be invisible by 2 weeks and find that it is not. The reassurance is that the pink-and-raised phase is the normal scar maturation curve — collagen is being deposited and remodeled, and the appearance will change substantially over the next 4 to 8 weeks. Patients are advised to protect the area from sun exposure (the pink phase is photosensitive and excessive sun can produce permanent pigmentation), avoid scratching or manipulation of the scar, and apply silicone-based scar gel as directed by the surgeon.
Week 6 to 8: The Transitioning Awkward Stage
Between week 6 and week 8 the scar begins to mature but is in an in-between phase that some patients find aesthetically awkward. The pink hue is lightening but not gone, the incision is flattening but still distinguishable, and the overall inner-corner appearance does not yet match the desired final result. Foreign patients who have been home for several weeks at this point may be tempted to message the clinic with concerns. The standard answer is to be patient through the awkward stage because the maturation curve continues to flatten and lighten the scar over the next 4 to 6 weeks.
Week 12: Matured Scar Along Natural Shadow Line
By week 12 the scar has matured to a near-final appearance. In properly performed epicanthoplasty with appropriate technique selection, the scar at week 12 is barely visible — it sits along the natural shadow line of the inner-eye contour where it blends with the existing eye anatomy. Patients viewing themselves in normal lighting do not see the scar without specifically looking for it. Close-up photographs in harsh light may reveal a fine line, but the scar is no longer a feature of the patient’s everyday appearance.
The scar continues to fade and flatten gradually through month 6 to 12, and the final appearance is typically reached between month 9 and month 12. Patients who evaluate the final result before month 6 are evaluating an incomplete maturation. The procedure deserves to be judged at the appropriate timeline.
Foreign Patient Travel Window
The standard recommendation is to stay in Seoul for 7 to 10 days, covering the day-0 surgery, day-5-to-7 suture removal, and one follow-up appointment after suture removal to confirm normal healing. Patients flying home day 8 to 10 typically have mild residual swelling that is not socially obvious if they wear sunglasses, and the scar at this stage is in the early pink phase that resolves with continued home recovery.
Patients who combine epicanthoplasty with double eyelid surgery and want maximum reassurance often extend the stay to 10 to 14 days to include a second post-operative check. Patients adding additional procedures on the same trip (rhinoplasty, fat grafting, or other procedures) typically extend to 14 to 21 days based on the recovery requirements of the additional procedures. The 12-week scar maturation continues at home with remote follow-up by photograph, which is standard at Korean clinics serving international patients.
Section 5: Verifying the Seoul Clinic and Foreign Patient Cost Comparison

The verification framework for choosing a Seoul clinic to perform epicanthoplasty centers on whether the surgeon treats the procedure as an anatomical decision or as a standardized service. The five-question verification checklist below covers the key signals.
Question 1: Which of the Four Standard Techniques Do You Recommend, and Why?
Ask the surgeon during consultation which technique they recommend for your fold and what about your specific anatomy makes that technique appropriate. An anatomically grounded answer references your fold thickness, your existing or planned crease angle, your lacrimal caruncle position, and your intercanthal distance. A standardized-service answer references the clinic’s “house technique” or “what we always do” without anatomical reasoning. The difference reveals whether the surgeon is performing structural assessment or applying a default procedure.
Question 2: Can I See 6+ Month Healed Photos of Your Own Epicanthoplasty Cases?
Photos at month 6 or later are the diagnostic standard because they show the matured scar and the stable final result. Photos at week 4 or week 8 are not yet matured and can make a poor result look acceptable. Request photos at month 6 minimum, ideally with patients of similar fold anatomy to your own. A surgeon with high case volume should have a substantial portfolio of healed cases. A surgeon who shows only early-stage photos or who deflects the request is signaling that the long-term results may not match the early appearance.
Question 3: What Conditions Trigger Reverse Epicanthoplasty in Your Practice?
Asking about revision and reverse procedures forces the surgeon to engage with the failure modes of the procedure. A surgeon who has a clear framework for when reverse epicanthoplasty is indicated, and who candidly acknowledges that over-correction is a possible outcome that they actively design to avoid, is signaling a mature understanding of the procedure. A surgeon who claims they never need to perform reverse procedures or who deflects the question is either over-confident or not engaging with the realistic outcomes of their own work.
Question 4: Will the Surgeon I’m Consulting Be the Surgeon Who Performs My Operation?
Consultation-and-operation continuity is the standard at clinics serving foreign patients but is not universal across all Korean clinics. Some clinics use senior surgeons for consultations and junior surgeons for operations, particularly for high-volume standardized procedures. The patient should explicitly confirm that the consulting surgeon will be the operating surgeon. Clinics that cannot or will not provide this continuity are signaling a workflow that prioritizes consultation volume over surgical outcome.
Question 5: What Is Your Approach to Foreign Patient Follow-Up After Departure?
Foreign patients leave Seoul before the scar fully matures and need a structured follow-up protocol to ensure normal healing and address any concerns. A clinic with a clear remote follow-up framework (typically photograph-based check-ins at week 2, week 6, week 12, and month 6) is signaling that they treat foreign patients as a long-term care relationship rather than a one-time procedure. Clinics without a remote follow-up protocol leave foreign patients without recourse during the awkward scar maturation phase.
Foreign Patient Cost Comparison
Korean epicanthoplasty pricing reflects clinic operating costs, currency, and very high case volume rather than any compromise on technique. The pricing table below covers the most common configurations.
| Region / Configuration | Typical Cost | Notes |
|---|---|---|
| Seoul — Standalone Epicanthoplasty | KRW 1,200,000–2,500,000 (USD 890–1,850) | Single procedure, 7–10 day stay, suture removal day 5–7 |
| Seoul — Combined with Double Eyelid Surgery (Suture / Partial Incision) | KRW 3,500,000–5,000,000 (USD 2,590–3,700) | Most common foreign patient package, 10–14 day stay |
| Seoul — Combined with Full Incision Double Eyelid + Ptosis Correction | KRW 5,000,000–7,500,000 (USD 3,700–5,560) | Comprehensive eye-shape package, 14–21 day stay |
| Seoul — Reverse Epicanthoplasty (Revision) | KRW 3,000,000–5,500,000 (USD 2,220–4,080) | Revision procedure for over-correction, 14–21 day stay |
| USA — Lateral Canthoplasty (Cosmetic) | USD 3,500–6,500 | Anatomically different procedure, not directly comparable |
| USA — Combined Double Eyelid + Inner Corner | USD 7,500–14,000 | Variable by surgeon training in Asian eye anatomy |
| Singapore / Hong Kong — Comparable Combined Package | SGD 8,000–14,000 (USD 5,900–10,300) | Higher operating cost, similar technique |
| Other Asia (verification critical) | USD 500–1,500 | Lower-tier clinics may apply standardized technique without anatomical assessment |
The pricing includes consultation, the procedure itself, and post-operative care through suture removal and the in-Seoul follow-up appointment. Patients should also budget for accommodation (typically USD 100 to 300 per night in Gangnam or central Seoul depending on hotel tier), airport transfers, post-operative medications and supplies, and meals. Hotel selection that allows easy walking-distance access to the clinic and to soft-food restaurants is a meaningful comfort consideration for the first week of recovery.
Coordinated Same-Trip Combinations
Foreign patients commonly combine epicanthoplasty with other procedures on the same trip to maximize travel value. Common pairings include rhinoplasty (the eye and the nose are the two highest-volume Korean facial procedures and the combination produces coordinated mid-face refinement), fat grafting to under-eye or temple regions (which addresses a different anatomical issue but synergizes with the eye-shape work), and selected skin treatments such as Rejuran skin booster therapy or similar texture treatments that can begin once the surgical recovery is past the initial healing phase.
Patients combining procedures should understand that the total recovery time extends beyond the longest single procedure and that the surgeon will design the operative sequence to minimize cross-interference. Eye procedures typically come first because the surgical field is small and healing is fast, with longer-recovery procedures (rhinoplasty, body contouring) added subsequently. The full coordination is mapped during consultation and adjusted based on the patient’s anatomy and trip length. The full Korean eye surgery category covers the related anatomical procedures that pair most often with epicanthoplasty on a single Seoul trip.
Frequently Asked Questions
Is Korean epicanthoplasty just for making eyes bigger?
No. Korean epicanthoplasty is an anatomical procedure that releases the Mongolian epicanthal fold, the skin web that covers the lacrimal caruncle (the inner pink corner of the eye). The visible result is wider inner intercanthal exposure and a softer inner-eye angle, but the surgeon is not making the eye bigger. The eye dimension itself does not change. What changes is the proportion of pink caruncle visible relative to the skin coverage. Foreign patients often misunderstand this as a Western “making the eye larger” procedure, but Korean surgeons treat it as a structural release that allows a separately performed double eyelid line to flow naturally into the inner corner without being competed against by the fold.
Will I have a visible scar from epicanthoplasty?
The scar is the central technical concern for epicanthoplasty, and the answer depends on technique selection and surgeon skill. With a well-executed Park Z-plasty or root Z-plasty placed along the natural shadow line of the inner-eye contour, the scar is barely visible at 12 weeks and typically not visible at all at month 9 to 12 once full maturation completes. The scar may appear pink, raised, or slightly visible during the first 6 to 8 weeks, which is the awkward stage that foreign patients sometimes worry about. Aggressive techniques or scars placed off the natural shadow line can be visible long-term. The verification step is asking the surgeon during consultation which technique they recommend for your fold and where the scar will sit, then comparing the answer against the surgeon’s actual healed photos at 6+ months.
Do I have to combine epicanthoplasty with double eyelid surgery?
No, standalone epicanthoplasty is a legitimate procedure for patients who already have a natural or surgical double eyelid but find their inner corner still covered by the Mongolian fold. About 15 to 25 percent of Korean epicanthoplasty consultations are standalone procedures. The pairing logic applies when a patient is also undergoing primary double eyelid surgery, because the new crease can be pulled downward by an unaddressed fold. If you already have a settled double eyelid, the question becomes whether the epicanthal fold by itself is competing with your existing crease or causing the inner-eye angle to look forced.
What if I already had double eyelid surgery elsewhere? Can I still add epicanthoplasty later?
Yes, and this is one of the most common standalone epicanthoplasty case profiles. Patients who had double eyelid surgery without epicanthoplasty often find at 6 to 12 months that the crease looks shortened or that the inner end of the crease appears covered by the residual fold. A separately staged epicanthoplasty can address this, and the technique selection accounts for the existing crease position so that the new release flows naturally into the established line. The recovery is identical to a standalone primary epicanthoplasty, and most Korean surgeons prefer to wait at least 6 months after the original double eyelid surgery before adding the epicanthoplasty so that the crease has fully matured.
How long should I stay in Seoul for epicanthoplasty?
The minimum is 7 to 10 days from arrival to departure. The surgery is day 0. Sutures are removed day 5 to 7. Most patients are comfortable flying home day 8 to 10 with mild residual swelling that is not socially obvious if you wear sunglasses. The 7 to 10 day window covers the suture removal, one post-suture follow-up appointment, and the worst of the visible swelling. Patients who want to be more conservative or who are combining epicanthoplasty with double eyelid surgery often stay 10 to 14 days. Patients who book back-to-back procedures (such as adding rhinoplasty or fat grafting on the same trip) typically extend to 14 to 21 days. The scar maturation timeline of 12 weeks continues at home with remote follow-up by photograph, which is standard practice at Korean clinics that serve international patients.
What does Korean epicanthoplasty cost compared to Western inner-corner procedures?
Standalone epicanthoplasty in Seoul typically runs KRW 1,200,000 to 2,500,000 (USD 890 to 1,850). When combined with double eyelid surgery the package price is typically KRW 3,500,000 to 6,000,000 (USD 2,590 to 4,440) depending on the double eyelid technique (suture, partial incision, or full incision) and whether ptosis correction or lateral canthoplasty is added. Western inner-corner procedures are not directly comparable because the Western technique is anatomically different, but typical Western lateral canthoplasty or canthopexy pricing for cosmetic indication runs USD 3,500 to 6,500. The pricing difference reflects clinic operating costs, currency, and the very high volume of epicanthoplasty cases that Korean clinics perform annually rather than any cut corner on technique.
Can epicanthoplasty be reversed if I don’t like the result?
Reverse epicanthoplasty exists as a revision procedure and is performed by experienced Korean revision surgeons. It is not a simple reversal because the original procedure removed a small amount of skin web and the revision must rebuild a fold using local skin flaps or careful suturing. The reverse procedure is more technically demanding than the original epicanthoplasty and is reserved for patients with significant over-correction (visible tear duct, unnatural rounded inner corner, or scar that pulls the inner eye into an unnatural angle). The best protection against needing a reverse procedure is conservative initial design, which is why the four-technique decision framework matters so much during the original consultation. A surgeon who recommends the minimum release necessary for the patient’s anatomy is more likely to produce a result that does not need reversal.
Will the scar be visible if I wear eyeliner or eye makeup?
By month 3 to 6, the scar is typically positioned along the natural shadow line of the inner-eye contour and is barely visible without makeup. Eyeliner applied along the upper lash line will not interact with the epicanthoplasty scar because the scar sits at the inner corner, not along the lash line. Patients who wear inner-corner highlighter (a common Korean and Asian eye makeup technique that emphasizes the lacrimal caruncle) often comment that the epicanthoplasty result makes this makeup approach more effective because the caruncle is more visible to begin with. Concealer is not typically needed after month 3, but during the first 4 to 6 weeks some patients use a small amount of mineral concealer over the pink scar phase if they want to look fully recovered for events or work.
What is the difference between epicanthoplasty and a “cat eye” procedure?
The “cat eye” aesthetic typically refers to lateral canthoplasty or lateral canthal lift, which lifts and tilts the outer corner of the eye upward. This is a separate procedure that targets the outer corner, not the inner corner that epicanthoplasty addresses. Some patients combine inner-corner epicanthoplasty with lateral canthoplasty to achieve a wider and slightly tilted eye shape, but the two procedures address different anatomy and have different recovery and scar concerns. Korean surgeons generally discourage aggressive lateral canthoplasty for Asian patients because the Asian outer canthal anatomy responds differently to the procedure than Western anatomy, and over-tilting can produce an unnatural look. The “cat eye” question during consultation often opens a separate discussion about whether the patient actually wants the cat-eye outer effect or simply wants the inner corner exposure that epicanthoplasty alone delivers.
How do I evaluate whether a Seoul clinic does epicanthoplasty well?
The evaluation criteria are specific. First, ask the surgeon during consultation which of the four standard techniques (Park Z-plasty, root Z-plasty, V-W plasty, or modified skin redraping) they recommend for your fold and why. A surgeon who answers with the anatomical reasoning (your fold thickness, your existing crease angle, your lacrimal caruncle position) is treating it as an anatomical decision. A surgeon who answers “we always do X” regardless of patient anatomy is treating it as a standardized service. Second, ask to see 6+ month healed photos of the surgeon’s own epicanthoplasty cases, ideally with patients of similar fold anatomy to yours. Third, ask about revision rates and what conditions trigger reverse epicanthoplasty in their practice. Fourth, verify that the surgeon performing your consultation is the same surgeon who will perform the operation, which is the standard at clinics serving foreign patients but is not universal across all Korean clinics. The four questions together filter for the surgeons who treat epicanthoplasty as the structural procedure it actually is.
Closing
Korean epicanthoplasty is not a cosmetic widening procedure that any patient can request on a menu. It is a structural release of the Mongolian epicanthal fold that Korean surgeons treat as a complement to double eyelid surgery in the 60 to 75 percent of consultations where the fold will interfere with the planned crease, and as a standalone procedure in the 15 to 25 percent of consultations where the patient already has a settled crease but a covered inner corner. The four standard techniques (Park Z-plasty, root Z-plasty, V-W plasty, and modified skin redraping) exist because no single approach fits every fold, and the surgeon’s job is to read the patient’s specific anatomy and select the technique accordingly. The scar matters more than the release itself because the procedure is judged on the matured 12-week appearance rather than the early healing phase, and well-executed technique places the scar along the natural shadow line where it is barely visible at maturation. Foreign patients who run the five-question verification framework during consultation, who understand the realistic 12-week timeline, and who treat the surgeon’s anatomical reasoning as a primary signal of quality are positioned to get the result the procedure was designed to deliver. Patients who book on price alone, or who treat epicanthoplasty as an upsell rather than as a structural decision, sometimes get a different result. For the full Korean eye surgery framework that contextualizes epicanthoplasty alongside the related anatomical procedures, visit Link Plastic Surgery’s official website.