The patient sat in the consultation room with a phone in her hand and tears in her eyes. She had flown in from Bangkok six weeks after a double eyelid surgery that left her with one fold sitting noticeably higher than the other, a scar band tugging her left lid open even when she tried to relax, and a heaviness across her brow she could not stop noticing in mirrors. She wanted surgery booked for that week. The senior surgeon, after a thirty-minute examination involving measurements she had never heard of, told her something she did not expect to hear in Seoul: come back in four to five more months. The consultation at Link Plastic Surgery is structurally different from what most foreign revision patients expect, and that difference begins with the calendar, not the scalpel.
This scene plays out almost weekly in Seoul revision clinics. Patients fly in from Bangkok, Manila, Sydney, Jakarta, and Singapore expecting that the world capital of eyelid surgery will fix in a week what their hometown clinic broke in a single afternoon. Instead they are told to go home, wait, manage their scars, and return. The wait is not punishment, not gatekeeping, and not a marketing trick to charge for two consultations. It is an anatomical reality that the foreign revision industry has largely refused to communicate honestly, and understanding why is the first step toward a revision that actually holds.

Why Seoul Surgeons Will Not Operate on Most Foreign Revision Patients Right Away
The patient with the high left fold was confused when she heard the timeline. Her primary surgery had been six weeks earlier. She had taken the time off work. She had paid for flights. She had assumed that being in Korea meant the problem would be addressed promptly. The surgeon walked her through what was happening under her skin, and the conversation reframed everything.
Scar tissue does not stay the same. In the first few weeks after surgery the wound is held together by fragile collagen and a population of cells called myofibroblasts, which are responsible for contracting tissue as it heals. Between weeks six and twelve those myofibroblasts reach their peak activity. The tissue is at its most reactive, most contractile, and most unpredictable. Operating into that environment is operating into a moving target. A revision performed at week six might look perfect on the operating table, then continue to contract and distort over the following months as the existing scar finishes its remodeling cycle alongside the new incision.
Seoul revision surgeons learned this through painful repetition during the medical tourism boom of the late 2010s. Patients flew in, demanded fast revisions, got them, and returned a year later with results that had drifted in ways the surgeon could have predicted but the patient had refused to wait for. The protocol that emerged from that experience is now nearly universal among established revision practices in Gangnam and Sinnonhyeon. Minimum six months from the primary surgery. Ideally nine to twelve months. Not flexible. Not adjustable for travel convenience. Not waived for celebrity status. The revision specialists at Link PS approach this differently from clinics that will book a revision the same week, because the underlying tissue biology does not change just because a patient bought a non-refundable plane ticket.
The Bangkok patient came back five months later. The scar band that had been tethering her left lid had softened considerably during the wait, partly because of a silicone gel protocol and partly because time had simply done what time does to scar tissue. The revision she ultimately had was significantly less invasive than what would have been required at six weeks, and the result settled cleanly within four months. She told the surgeon afterward that she had been furious about the wait. She also said she would never go back.
Three Anatomical Realities That Make Revision Different from Primary
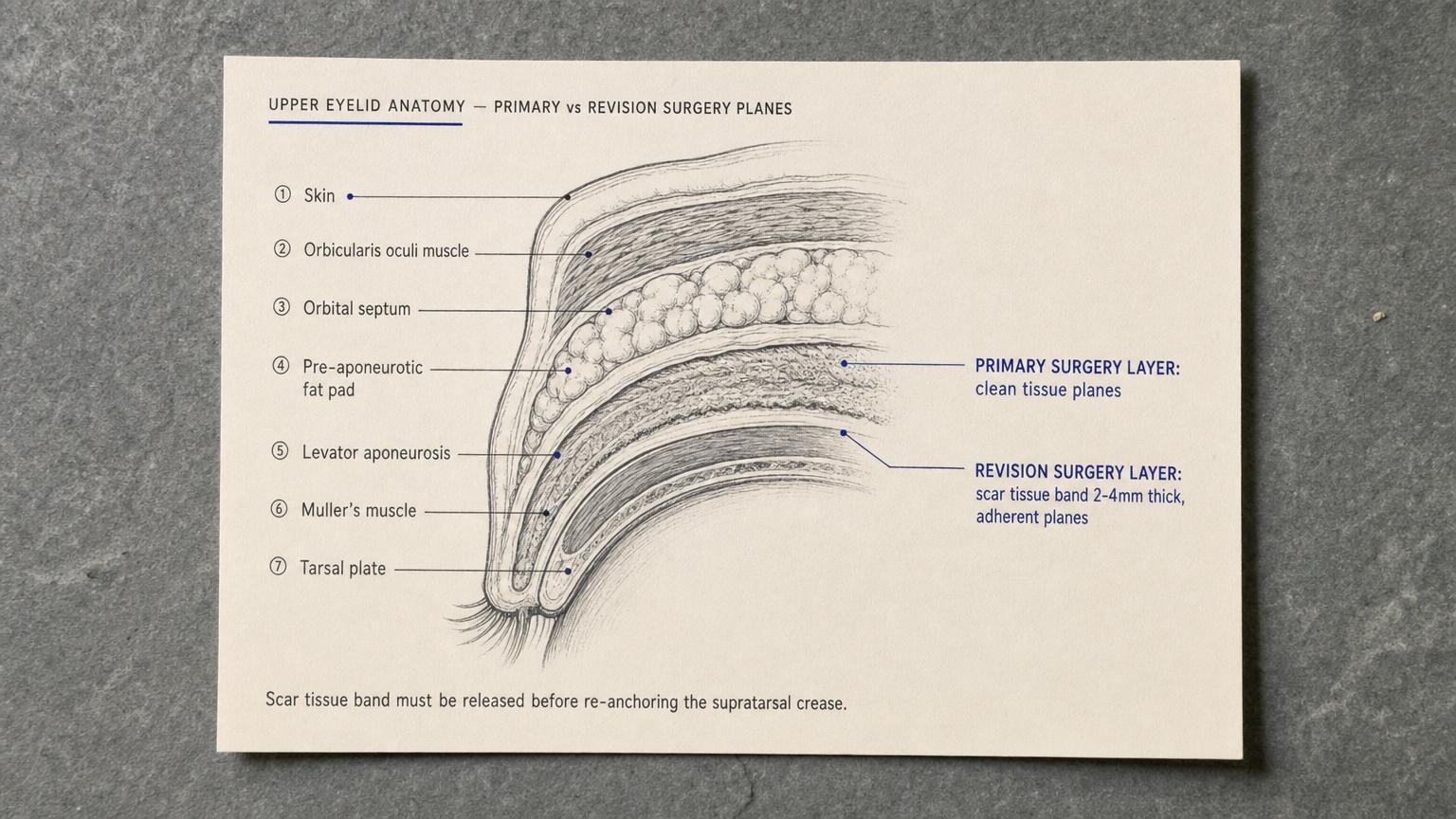
A primary double eyelid surgery operates on virgin tissue. The planes are clean, the fat pads sit where the textbook says they should, and the levator aponeurosis (the thin sheet of tissue that lifts the upper lid) is at its normal thickness and attachment. Revision surgery operates on tissue that has been cut, sutured, and remodeled at least once. The same anatomical philosophy applies whether the primary was a double eyelid procedure or comprehensive lid surgery, but the surgical environment is profoundly different from primary anatomy, and the surgeon must account for three specific changes before deciding what is actually possible.
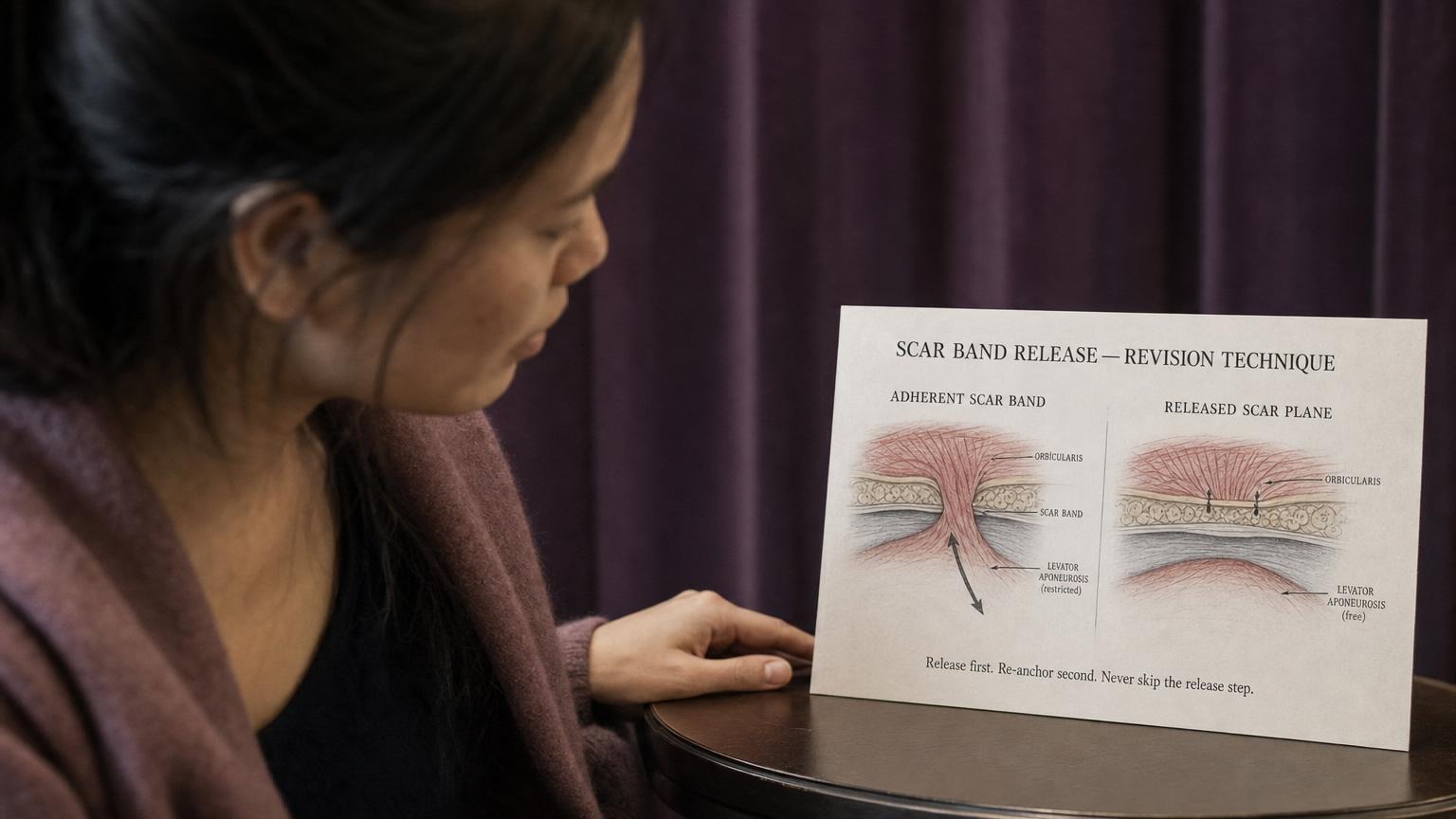
The first reality is the adherent scar band. When the primary surgery healed, the deep tissue of the lid often formed adhesions to the levator muscle that pulls the lid open. This is normal, and in many cases it is what creates the fold. The problem arises when the adhesion is in the wrong place, pulls at the wrong angle, or tethers the levator so tightly that the lid cannot close completely. You cannot just recut the skin and expect the fold to behave. The scar band itself has to be identified, dissected free, and released along its full length. A surgeon who only revises the skin without releasing the deep adhesion produces a result that looks better for three weeks and then reverts.
The second reality is pre-aponeurotic fat displacement. The fat pad that sits in front of the levator aponeurosis is supposed to provide a soft cushion between the levator and the skin. During primary surgery this fat is often partially removed, redistributed, or pushed into a position that does not match the original anatomy. By the time revision is considered, the fat may have settled into a configuration that creates the visible problem (a hollow upper sulcus, an unnatural ridge, a fullness that looks wrong). Revision requires identifying where the fat has gone, deciding whether to move it, leave it, or supplement it with grafted fat, and then committing to that plan before any sutures go in.
The third reality is levator aponeurosis attenuation. When a primary surgeon places sutures through the levator to fix the fold, the levator can stretch, thin, or partially dehisce from its normal attachment to the tarsal plate. The result is often a subtle ptosis (a droop of one or two millimeters) that the primary surgeon did not diagnose and the patient did not notice because the eyelid surgery itself dominated the visual change. By the time revision is considered, this attenuation is contributing to the asymmetry the patient sees. A revision that ignores the levator and only fixes the skin will leave the underlying ptosis untouched, and the asymmetry will persist no matter how perfectly the new fold is placed.
Korean revision standards require all three of these realities to be identified, documented, and addressed in the surgical plan before the scalpel touches the skin. Foreign primary clinics often do not have this framework, partly because they see revision rarely, partly because their training tradition focused on primary aesthetics, and partly because a fifteen-minute consultation cannot uncover what a thorough revision workup requires.
MRD1, Levator Function, and Skin Inventory: The Seoul Diagnostic
The thirty-minute diagnostic the Bangkok patient went through is not a Korean invention. The measurements involved (MRD1, levator excursion, pinch testing, vector analysis) are standard in academic oculoplastic surgery worldwide. What is distinctly Korean is the insistence on performing all of them, in sequence, on every revision patient, before any surgical plan is offered. Seoul’s blepharoplasty approach uses the same MRD1 framework across primary and revision cases, but in revision the diagnostic discipline becomes load-bearing.
Recommended for Your Recovery
Products commonly used before and after Korean eye revision — same items routinely recommended in the recovery instructions Seoul clinics hand out at discharge.
- Arnica Montana Tablets — begin 3 days before eyelid surgery to reduce periorbital bruising and swelling. Check price on Amazon
- Gel Eye Mask (Cold Compress) — reusable cold pack for the every-two-hour icing schedule on day 1 to day 3. Check price on Amazon
- Silicone Scar Sheets — apply from week 3 onward along the upper lid incision line if your procedure was incisional. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — lightweight Korean sunscreen to protect the healing scar and prevent post-inflammatory pigmentation. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
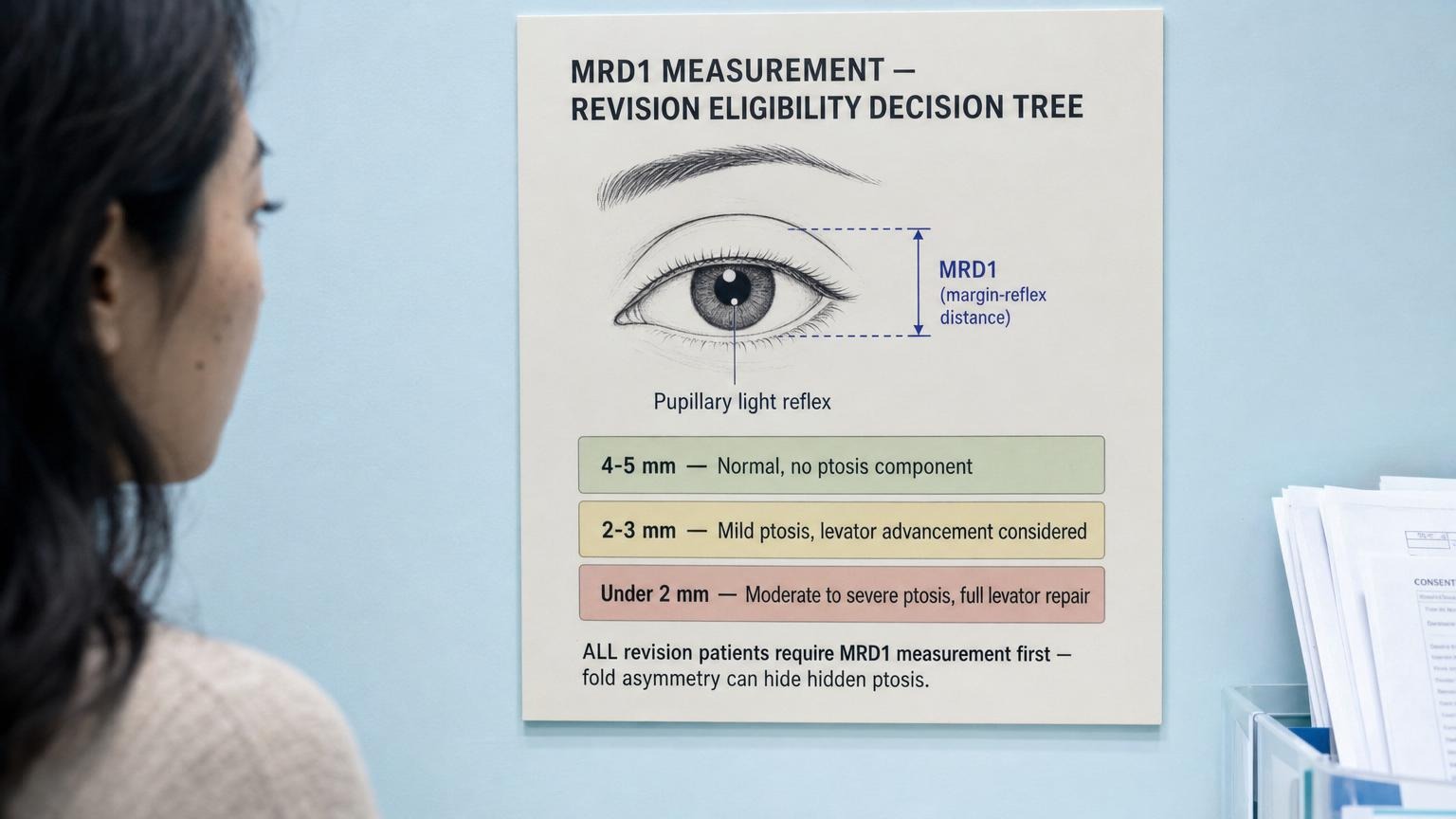
MRD1 stands for marginal reflex distance 1. It measures the distance from the corneal light reflex (the bright dot that appears when a light is shone at the eye) to the margin of the upper eyelid. In a normal adult eye the MRD1 is approximately four to five millimeters. A patient with mild ptosis will measure two to three millimeters. Moderate ptosis is anything less than two. Severe ptosis is below one millimeter, with the lid sitting on or below the pupil. The measurement is taken with the patient looking straight ahead, the brow gently held still to prevent compensatory lifting, and the light positioned at exactly the right distance.
The reason this matters for revision is that most foreign revision patients have undiagnosed mild ptosis from their primary surgery. The primary surgeon focused on creating the fold and did not notice (or did not communicate) that the levator had been weakened in the process. The patient sees asymmetry and assumes the fold is the problem. The revision surgeon measures MRD1 and discovers that one side is three millimeters and the other is four. Now the surgical plan changes completely. Revising the fold without correcting the underlying ptosis will reproduce the asymmetry no matter how perfectly the new fold is placed.
The levator function test follows MRD1. The patient is asked to look down, then up, while the surgeon holds the brow still and measures the excursion of the upper lid margin. Normal excursion is twelve to fifteen millimeters. Reduced excursion (under ten millimeters) indicates a levator that is not functioning at full capacity. This finding changes the surgical approach. A patient with good levator function can usually be revised with a conventional levator advancement. A patient with reduced function may need a different technique entirely (Müller muscle conjunctival resection, frontalis sling, or a graded approach depending on severity). This diagnostic discipline mirrors the revision rhinoplasty protocol in which structural diagnosis precedes any commitment to a surgical plan, and for the same reason: revision is not a redo, it is a different operation built on different assumptions.
Skin inventory is the third pillar. The surgeon uses a pinch test to measure how much skin can be removed without compromising lid closure. Vector analysis assesses whether the brow position is contributing to the apparent eyelid problem (a low brow can make a normal lid look heavy, and revising the lid without addressing the brow will leave the patient unhappy). Tarsal plate height is measured to determine how high the new fold can realistically be placed without creating a staring or surprised appearance. All of this takes approximately thirty minutes. Foreign primary clinics frequently complete the entire consultation in fifteen, which explains a great deal about why their patients eventually fly to Seoul.
The Six-Month Wait Protocol Foreign Patients Hate, and Why It Works
The protocol that emerges from this diagnostic framework is structured around scar maturation rather than patient convenience. Month zero is the consultation, full photographic documentation, and the measurements described above. The surgeon explains what is anatomically present and what the plan will be once the tissue is ready. The patient is given a scar management regimen and a return date.
Months one through three are the scar maturation phase. The patient applies medical-grade silicone gel to the existing incision line twice daily. Sun protection is enforced with SPF 50 or higher, because ultraviolet exposure during this window can permanently darken the scar. Gentle massage along the scar line begins around week eight, using upward and outward strokes for approximately two minutes per session, two to three times per day. The patient does not see the surgeon during this phase but sends photos at monthly intervals so the team can track scar softening.
Month four is the re-evaluation. The patient returns either in person or via a structured video consultation. The surgeon assesses scar pliability (using a standardized scale), takes new measurements, and finalizes the surgical plan. If scar maturation is on track, surgery is scheduled. If maturation is slower than expected (which happens in roughly fifteen percent of cases), the wait extends another two months. The patient does not get to override this decision.
Month six is the surgery window. By this point the scar has reached approximately seventy to eighty percent of its final maturity. Myofibroblast activity has declined to baseline. The tissue planes can be dissected cleanly. The levator can be advanced predictably. The fold can be placed with confidence that it will hold. The surgery itself is often shorter than the primary, because the diagnostic work has already been done and the surgeon knows exactly what needs to happen.
Patients hate the wait. They feel that six months is a punishment for having chosen the wrong surgeon the first time. They calculate the lost time, the disrupted social life, the months of avoiding mirrors. The frustration is real and the team does not dismiss it. What they do communicate, repeatedly and in writing, is the data that justifies the protocol. Published Korean revision data shows revision success rates around eighty-seven percent when the six-month protocol is followed. Early revisions (performed at six to twelve weeks) show success rates closer to fifty-four percent, with a much higher rate of needing a third surgery within two years. The wait is the difference between a revision that holds and a revision that becomes the second mistake in a sequence.

Cost and What Korean Revision Actually Includes
Pricing for Korean eye revision varies by complexity. A straightforward fold-only revision (no ptosis correction, no scar band release, minimal fat repositioning) typically falls in the range of four to five million Korean won. A comprehensive revision involving fold reconstruction, levator advancement, fat repositioning, and scar band release runs five to seven million won. Revisions involving previous canthal surgery (epicanthoplasty or lateral canthoplasty gone wrong) can exceed seven million when significant tissue reconstruction is needed.
| Region | Revision Price Range | Notes |
|---|---|---|
| Korea (Seoul) | KRW 4.0M to 7.0M (USD 3,000 to 5,200) | Includes 6-month follow-up, scar protocol, 12-month re-revision warranty |
| Thailand (Bangkok) | THB 90,000 to 140,000 (USD 2,500 to 3,900) | Follow-up and warranty terms vary widely |
| USA | USD 8,000 to 14,000 | Oculoplastic specialist; revision often more than primary |
| Australia | AUD 12,000 to 18,000 | Limited revision specialists outside major cities |
What the Korean revision price typically covers is broader than what foreign patients are used to. The fee includes the six-month structured follow-up (in person if possible, video consultation otherwise), the scar management protocol with provided materials, and a re-revision warranty if a third surgery becomes necessary within twelve months of the revision. The warranty is real and is documented in the consent paperwork. Foreign primary clinics rarely offer twelve-month re-revision warranties, partly because revision is not their core practice and partly because the underwriting math does not work for low-volume operators.
Before committing to any clinic, foreign patients can verify the revision protocol with five direct questions. Does the clinic require a minimum six-month wait from the primary surgery, and what is the policy if maturation is slower than expected? Will the surgeon measure MRD1 and document it in writing during the consultation? Is the scar tissue assessment provided as a written report, including specific findings about adhesion, fat displacement, and levator function? What are the specific terms of the re-revision warranty, including the window, the conditions, and what is excluded? Who manages remote follow-up after the patient returns home, and how often are check-ins scheduled? A clinic that hesitates on any of these questions is not the right clinic for a revision case. To explore other eye procedures and understand the broader context of Seoul eye surgery, the categorized hub pages provide a structured starting point.

Frequently Asked Questions
1. Is the six-month wait period flexible? My travel schedule is tight.
The six-month wait is based on tissue biology, not policy. Scar tissue is at peak myofibroblast activity between weeks six and twelve, and operating into that environment significantly increases the risk of a second revision. Some surgeons will consider a four-month minimum in selected cases with rapid scar softening, but six months is the typical floor. Patients who push for earlier surgery often regret it within a year.
2. What happens if my scar tissue does not soften enough by month six?
Roughly fifteen percent of revision candidates have slower than expected scar maturation. The protocol in that case is to extend the wait another two months, continue silicone gel and massage, and re-evaluate at month eight. Operating into immature scar to meet a schedule is the most common cause of failed revisions in this population.
3. Can ptosis correction be combined with the revision?
Yes, and in most foreign revision cases it should be. Undiagnosed mild ptosis from the primary surgery is one of the most common contributors to apparent fold asymmetry. The MRD1 measurement during consultation determines whether ptosis correction is needed. Combining the procedures is more efficient and produces better symmetry than doing them sequentially.
4. I had a non-incision primary. Does the same revision wait apply?
Slightly different. Non-incision (suture) primary surgeries produce less scar tissue, so the wait can sometimes be shortened to four months if examination confirms minimal deep scarring. However, if the non-incision primary failed because the underlying anatomy required an incision approach, the revision is essentially a primary incision surgery and follows primary protocols rather than revision protocols.
5. Does revision work differently for Asian versus Western eye anatomy?
The diagnostic framework is the same. The anatomical specifics differ. Asian eyelid anatomy typically has a lower position of the levator aponeurosis attachment and a larger pre-aponeurotic fat pad. Western eyelid anatomy has a higher levator attachment and less fat. Revision surgeons adjust the surgical plan accordingly, but the measurements taken and the wait protocol followed are identical regardless of ethnicity.
6. Why is revision typically more expensive than the primary surgery?
Revision requires longer operating time, more complex tissue dissection, and a surgeon with revision-specific training. The diagnostic consultation alone is longer than most primary consultations. Additionally, the warranty terms and structured follow-up included in revision pricing represent real costs that primary surgery does not carry. The price gap is generally twenty to forty percent.
7. Is recovery longer than the primary surgery?
Visible bruising and swelling timelines are similar to primary surgery (one to two weeks for the worst, three to four weeks to look reasonably normal in public). Final settling of the result is slower with revision, typically four to six months rather than the three to four months for primary. The longer timeline reflects the fact that scar tissue is layered (existing scar plus new scar) and remodels more slowly.
8. What is the risk that I will need a third surgery?
With the six-month protocol followed and a properly trained revision surgeon, published rates suggest approximately eight to thirteen percent of revision patients eventually need a third surgery, usually for minor refinement rather than major reconstruction. Without the wait protocol, rates climb above thirty percent. The wait is the single largest factor in avoiding a third surgery.
9. What anesthesia is used for revision?
Most Korean revision cases use local anesthesia with light sedation, the same approach as primary double eyelid surgery. The patient is comfortable, can respond to commands when the surgeon needs to assess fold position, and recovers quickly. General anesthesia is reserved for cases involving extensive reconstruction or combined procedures.
10. How long should I plan to stay in Seoul for the revision surgery itself?
Seven to ten days covers most revision cases. Day one is final consultation and preoperative testing. Day two or three is surgery. Days four through seven include suture removal (typically day five to seven) and the first postoperative photo documentation. Days eight through ten allow for any swelling adjustment and the final pre-departure check. After return, structured video follow-ups continue for the next six months. For travel planning details, visit Link Plastic Surgery’s official website for the most current scheduling information.