Korean Upper Eyelid Fat Removal: The Procedure for People Whose Eyes Look Tired Even When They Aren’t

Most foreign patients fly into Seoul wanting double-eyelid surgery and walk out of the consultation with a different surgical plan: upper eyelid fat removal — without creating a double-eyelid line at all. They explain to the surgeon that their eyes look heavy and tired, that mascara won’t stay, that even after eight hours of sleep their eyes still look swollen. The surgeon points at the soft pad of tissue sitting just above the lash line and says: “Your eyes don’t need a new fold. They need this layer of fat reduced.” This is the procedure Korean clinics call nun-kkeo-pul ji-bang je-geo — upper eyelid fat removal — and for the right patient it is the smallest, lowest-downtime, most under-the-radar eye procedure in the entire Korean cosmetic playbook.
This guide is for the patient who has searched “Korean blepharoplasty” or “Asian double-eyelid surgery” and felt like neither name describes what they actually want. You don’t want a new eyelid crease. You don’t want bigger eyes. You want the heavy, hooded, swollen-looking upper lid to look like it does after a really good night of sleep — except permanently. That’s exactly what this procedure does, and it’s the procedure that Link Plastic Surgery has quietly performed more than almost any other eye procedure on its standalone menu.
What Patients Actually Mean by “My Eyes Look Tired”
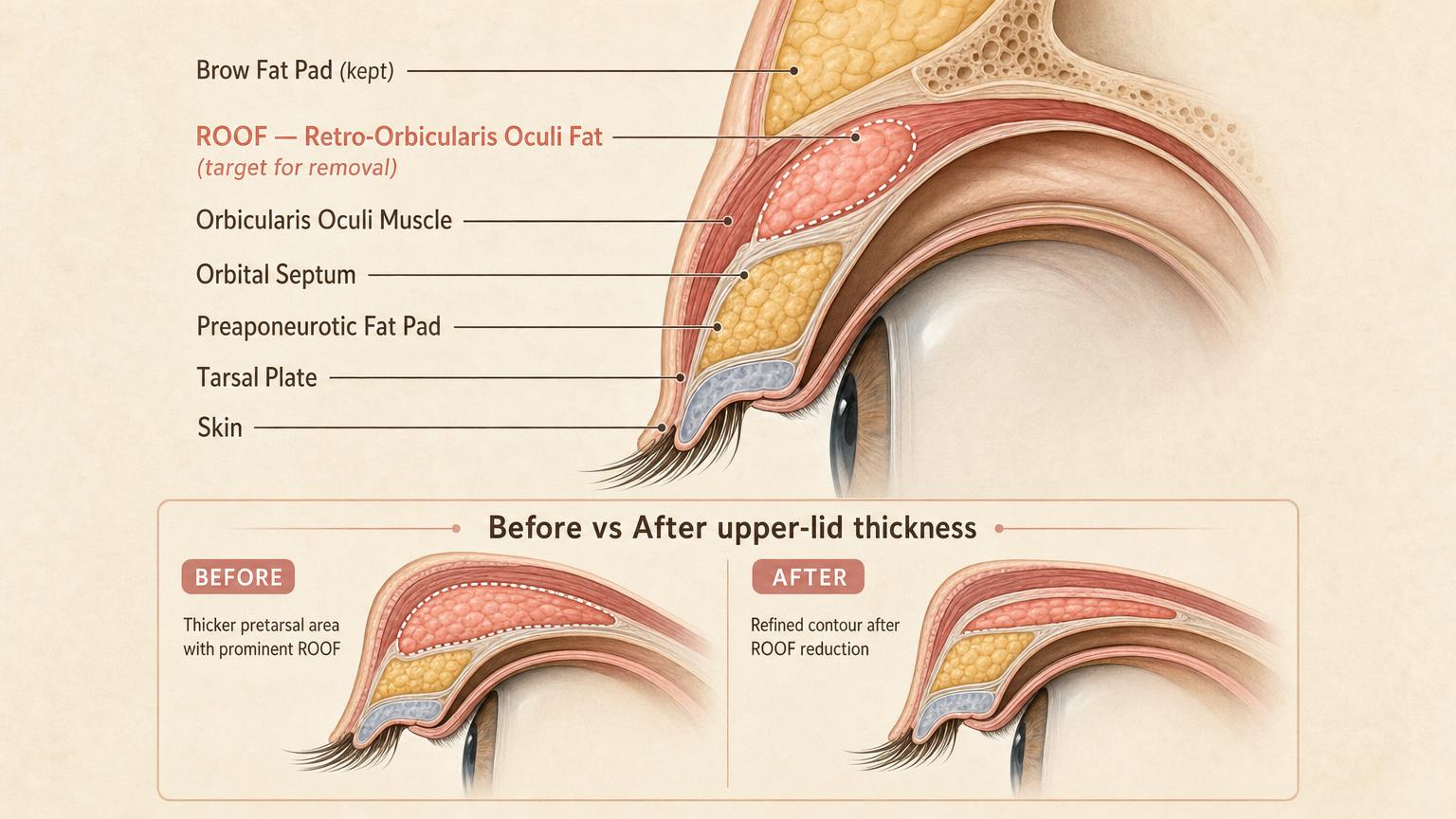
The complaint that brings most patients in is impossibly vague at first: “my eyes look heavy.” But once a Korean surgeon traces what’s anatomically happening, the patient usually recognizes the diagnosis immediately. There is a specific fat pad sitting just under the skin of the upper eyelid called the ROOF — Retro-Orbicularis Oculi Fat. It sits between the orbicularis muscle (the muscle that closes your eye) and the deeper structures, and in some people — particularly those with East Asian eyelid anatomy — this pad is thicker than average from birth or thickens with age. The result is what looks externally like a permanently puffy upper eyelid, even when you’re well-rested.
This is not the same problem as ptosis (a droopy upper lid caused by weak levator muscle) and it is not the same as excess upper-lid skin (the condition that creates true hooding in older patients). It is purely a soft-tissue fullness problem, and the surgical fix is correspondingly narrow: remove the ROOF (and sometimes a small amount of orbital fat), leave everything else alone. No skin removed. No double-eyelid crease created. No muscle altered. The eye shape stays exactly the same — just the puffiness goes away.
One Link Plastic Surgery patient described the realization moment in her cafe review: “My upper eyelids were always thick, and looked puffy when seen from the side. The price matched what I’d seen on Gangnam Unni, and the staff were all friendly. Even the anesthetic injection was less painful than I expected, and the swelling wasn’t bad — I was able to go back to normal life right away.” This is the recurring patient profile: someone who already knows the puffiness is congenital, who has tried every concealer and eyelid tape product on the market, and who finally realizes that surgical reduction is the only thing that actually solves the underlying anatomy.

Real Link Plastic Surgery patient — standalone upper eyelid fat removal, before and one-week post-op (anonymized eye-region close-up). Notice the puffy upper lid platform is visibly thinner, the eye crease (or lack of) is unchanged.
Another distinction worth understanding is how this contrasts with the standard Western blepharoplasty mindset. In US/UK practice, the dominant procedure for “heavy upper eyelids” is upper blepharoplasty — which primarily removes skin. That’s because the patient demographic in Western clinics skews older, and the predominant cause of upper-lid heaviness in 50+ year-old Caucasian patients is genuinely skin redundancy (dermatochalasis), not subcutaneous fat thickness. The Korean patient demographic seeking this procedure is much younger — often 25–40 — and the cause is almost always congenital ROOF fullness, not skin laxity. The same complaint (“my upper eyelids look heavy”) therefore points to two different anatomical problems and two different surgical solutions depending on age and ethnicity. Korean surgeons specifically train for the ROOF-driven version because it is overwhelmingly what walks through their clinic doors.
The Two Korean Surgical Approaches

Korean clinics use two distinct techniques for upper eyelid fat removal, and the choice between them is anatomical — not preference-based. A surgeon who only offers one of the two has not fitted the procedure to your specific eyelid.
Conjunctival Approach (Hidden Incision)
The conjunctival technique places the incision on the inside surface of the upper eyelid, completely hidden from external view. The surgeon everts the lid, makes a small incision through the conjunctiva, and removes the ROOF fat from the inside. The incision is closed with fine absorbable sutures that dissolve on their own — there is no external scar at any stage of healing. This technique is appropriate for:
- Younger patients with good upper-lid skin elasticity
- Mild to moderate ROOF excess without skin redundancy
- Patients who explicitly want zero external scarring above all else
- Patients who do not want any change to the existing eyelid crease (or absence of one)
The cosmetic advantage is obvious — nothing visible at any point. The structural limitation is that the conjunctival approach cannot address loose upper-lid skin, so it is the wrong technique if the patient also has excess skin that needs tightening.
Subbrow Approach (Brow-line Incision)
The subbrow technique places the incision along the lower edge of the eyebrow, hidden in the natural brow hairline. The surgeon removes the ROOF fat through this access point and can also tighten a small amount of upper-lid skin in the same procedure if needed. The healed scar lies along the brow line and is essentially invisible once the brow hair grows back over it. This technique is appropriate for:
- Patients in their late thirties and beyond who have both ROOF excess and some skin redundancy
- Cases where the heaviness comes from a combination of fat + skin (not fat alone)
- Patients who also want a subtle brow lift effect (the technique can lift the brow slightly as a side benefit)
- Patients who don’t mind a fully healed scar tucked into the brow hairline
A patient at Link Plastic Surgery’s eyelid fat removal page may be presented with either technique depending on the in-person evaluation. The decision is made after physically pinching the upper-lid skin and assessing both fat thickness and skin laxity simultaneously.
What This Procedure Is NOT
This is the part most foreign patients misunderstand. Upper eyelid fat removal is not:
- Not double-eyelid surgery. No crease is created. If you go in with a monolid, you come out with a monolid (just a less puffy one). If you go in with a double eyelid, your existing crease is preserved exactly as it was.
- Not ptosis correction. The droopiness of a true ptosis comes from the levator muscle, not from fat. Fat removal cannot fix ptosis.
- Not upper blepharoplasty. Standard upper blepharoplasty in Western practice removes mostly skin and sometimes a sliver of muscle. Korean ROOF reduction removes mostly fat and leaves skin intact (conjunctival approach) or removes minimal skin (subbrow approach).
- Not a brow lift. Though the subbrow variant produces a mild brow lift as a side effect, the primary surgical goal is fat reduction, not brow elevation.
For patients who actually do need any of the above, the surgical plan will combine techniques — and a Korean clinic that prefers honesty will tell you upfront which of these you genuinely need versus which are surgical upsells.
What Recovery Actually Looks Like

This is the recovery profile that surprises foreign patients most. Upper eyelid fat removal has one of the fastest recovery timelines in the entire Korean eye-surgery menu — significantly faster than double-eyelid surgery, ptosis correction, or under-eye fat repositioning. Here is the realistic timeline.
Recommended for Your Recovery
Products commonly used before and after Korean upper eyelid fat removal — same items routinely recommended in the recovery instructions Seoul clinics hand out at discharge.
- Arnica Montana Tablets — begin 3 days before eyelid surgery to reduce periorbital bruising and swelling. Check price on Amazon
- Gel Eye Mask (Cold Compress) — reusable cold pack for the every-two-hour icing schedule on day 1 to day 3. Check price on Amazon
- Silicone Scar Sheets — apply from week 3 onward along the upper lid incision line if your procedure was incisional. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — lightweight Korean sunscreen to protect the healing scar and prevent post-inflammatory pigmentation. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
Day 0 (Surgery Day)
The procedure itself takes 20–30 minutes. It is performed under local anesthesia only — no sedation, no general anesthesia, no IV. The surgeon injects a small amount of local anesthetic around the upper eyelid, and the patient remains fully awake and comfortable throughout. There is no admission, no recovery suite, no fasting requirement. Most patients walk out of the clinic within 90 minutes of arrival.
One cafe review captured the day-of experience: “On January 14th, Dr. Sung Ha-min performed the upper eyelid fat removal under local anesthesia. The staff and the doctor were all friendly, and the procedure ended quickly with no pain at all.”
Days 1–3
Mild swelling at the upper eyelids — visible but subtle. The rest of the face looks completely normal. There is no bandage (conjunctival approach has nothing to bandage) and no medical tape covers anything. Bruising is rare and, when it appears, is limited to a small area near the lid margin. Most patients are back to working from home or office within 24–48 hours.
Crucially, because there is no external incision (conjunctival approach), there is no concern about a wound getting wet, no special cleaning protocol, no risk of an obvious “I just had eye surgery” appearance in public. A patient who has the conjunctival approach can attend a meeting on day 2 and a casual observer would notice nothing unusual.
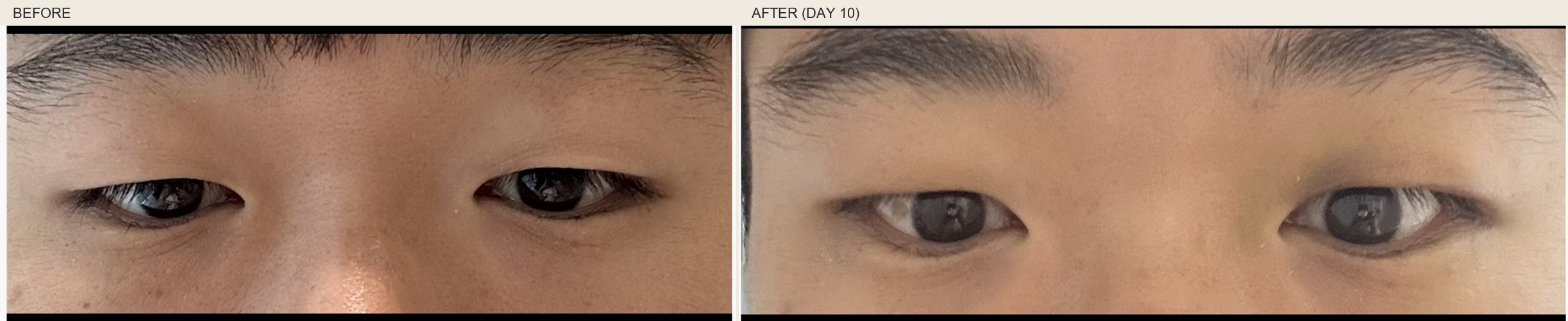
Another Link Plastic Surgery patient at day-10 post-op (anonymized close-up). The upper lid is visibly lighter with only minor residual color change near the lid margin — the kind of result that most observers read as “well-rested” rather than “post-surgical.”
Day 7 (Suture Removal)
If the subbrow approach was used, external sutures are removed at day 7 (a 5-minute clinic visit). If the conjunctival approach was used, there are no external sutures and this visit is optional. The internal absorbable sutures dissolve on their own over 2–4 weeks.
Days 8–14
Residual swelling continues to settle. The upper lids look lighter and more open than before surgery, but slightly tighter than the final result will be. Most patients return to full social life by day 8. Makeup including mascara and eyeshadow is permitted from day 8 (conjunctival) or day 10 (subbrow, to fully heal the brow incision).
Week 2 (Practical Final)

The upper eyelid contour looks essentially settled — visibly lighter, less hooded, more rested appearance. This is the stage at which patients say their friends notice “you look well-rested” or “did you change your makeup?” without identifying that surgery happened. The full settling continues over 1–3 months as the last traces of swelling resolve.
Month 3 (Final)
Final result is settled. The reduced upper-lid contour looks natural. Any subbrow scar (if used) is pink-and-fading at this point and continues to lighten over months 4–6. By month 6 the scar is typically invisible at conversational distance.
Cost, Standard of Care, and the Five Questions That Matter
The cost comparison between Korea and Western clinics for this specific procedure is significant — but for an interesting reason. Most Western clinics do not offer ROOF reduction as a standalone procedure at all. They either bundle it into a full upper blepharoplasty (which costs much more and removes skin you may not need to lose) or refuse to do isolated fat reduction because they aren’t trained in the conjunctival approach.
| Region | Standalone Upper Eyelid Fat Removal | Combined with Skin Excision (Upper Bleph) | Recovery Support |
|---|---|---|---|
| Korea (Seoul) | KRW 1.5–3M (USD 1,100–2,200) | KRW 2.5–4.5M (USD 1,850–3,300) | Suture removal + 2 follow-ups included; scar care kit provided |
| USA | Rare — usually bundled (USD 4,500–8,000 for full upper bleph) | USD 4,500–8,000 | Variable; follow-up often charged separately |
| UK / EU | Rare — usually GBP 3,000–5,000 as part of upper bleph | GBP 3,000–5,000 | Private clinics charge per visit |
| Australia | AUD 5,000–8,000 (usually combined) | AUD 5,000–8,000 | Limited follow-up window |
The price advantage is real, but more interesting is the availability advantage. A standalone conjunctival ROOF reduction (no skin removed, no external incision) is a procedure that genuinely struggles to be sourced outside of Korea and a handful of clinics in Japan. If you specifically want this — and not a full upper blepharoplasty — Korea is one of the few places that performs it routinely.
If you are flying in for this procedure, these are the five questions that separate clinics that know what they’re doing from those that don’t:
- Do you offer both conjunctival and subbrow approaches, and how do you decide between them for my anatomy? A clinic that only does one is fitting your face to their procedure rather than the reverse.
- Will the surgery affect my existing eyelid crease (or lack of crease)? The honest answer is no — fat removal alone should not change the crease. If a surgeon says they will “improve” the crease while removing fat, they are upselling double-eyelid surgery.
- Is this performed under local anesthesia only, or do you require sedation? Standalone ROOF reduction should be a local-anesthesia-only procedure. If a clinic insists on sedation, ask why — there is usually no medical reason.
- What is your protocol if I have residual asymmetry at 3 months? Minor asymmetry (one side slightly more reduced than the other) is the most common outcome that may need touch-up. Free revision within 6–12 months for surgical asymmetry should be standard policy.
- Can I see your own surgeon’s portfolio for this specific procedure? Not the clinic’s overall results — the specific surgeon’s standalone ROOF reduction cases. Standalone fat reduction looks different from full upper bleph, and you want to see that the surgeon does this exact procedure regularly.
This procedure pairs naturally with two other Korean specialty procedures that patients sometimes consider in the same visit: under-eye fat repositioning for patients who have both heavy upper lids and under-eye hollowing/bags, and Korean double-eyelid surgery for patients who want both the fat reduced and a new defined crease created. The decision to combine procedures is made at the in-person consultation and depends on the patient’s actual anatomy, not on what they thought they wanted before walking in.
Frequently Asked Questions
Will my eye shape change?
No — and this is the entire reason patients choose this procedure over double-eyelid surgery. Only the thickness of the upper-lid soft tissue is reduced. The eye opening, brow position, and existing crease (or monolid) are preserved exactly. People notice you look more rested without being able to identify what changed.
Can I have this if I already have a double eyelid?
Yes. If you have a natural or surgical double-eyelid crease but the upper lid is still puffy above the crease, the conjunctival approach can reduce the fat without touching the crease at all. This is a common combination request: existing double-eyelid + ROOF reduction.
Is the result permanent?
The ROOF fat that is removed does not regenerate, so in that sense yes. However, natural aging continues — over decades, gravity and skin laxity will produce age-related upper-lid changes regardless. Most patients enjoy the fat-reduced contour for many years before any retouch becomes a consideration.
What’s the difference between this and Western upper blepharoplasty?
Western upper blepharoplasty primarily removes skin and a sliver of muscle, addressing hooding caused by skin redundancy. Korean upper eyelid fat removal primarily removes ROOF fat, addressing puffiness caused by congenital or age-related fat thickness. They solve different anatomical problems. Younger Asian patients almost always need the Korean version, not the Western version.
How much fat is actually removed?
The amount is small — typically 0.5–1.5 mL of ROOF fat per side, plus occasional small amounts of orbital fat through the same access. The surgeon stops short of over-reduction because removing too much creates a hollowed, prematurely-aged upper-lid appearance that is very difficult to reverse. Conservative reduction is the Korean standard.
What if I have asymmetric upper lids before surgery?
Many patients do — congenital asymmetry of upper-lid thickness is common. The surgical plan accounts for this: the surgeon may remove slightly more fat from one side than the other to balance the result. The pre-surgical asymmetry should be discussed at the consultation and the surgical plan should explicitly address it.
Can men get this procedure?
Yes, and the patient population is more male-balanced than for double-eyelid surgery. Korean male patients commonly seek upper eyelid fat removal because they want the “tired-looking” complaint resolved without any visible cosmetic change — the procedure suits male preferences for invisible interventions particularly well.
Will I look hollow afterward?
This is the main complication patients worry about, and the answer comes down to surgeon judgment. Over-reduction of ROOF can create a hollowed, prematurely-aged contour. Korean surgeons trained in this procedure deliberately leave a small amount of fat in place to preserve a natural fullness — the goal is “rested” not “skeletal.” If a surgeon shows you portfolio images of patients with visibly hollowed upper lids, choose a different surgeon.
Can I add this to a Korean rhinoplasty or other procedure in one visit?
Yes. Standalone upper eyelid fat removal is a small enough procedure that it is commonly added to a larger surgical plan in the same operative session. Patients flying in for Korean rhinoplasty sometimes add eyelid fat removal in the same visit. The combined recovery is essentially the rhinoplasty recovery — the eyelid procedure adds minimal additional downtime.
Closing
Upper eyelid fat removal is the Korean eye procedure that foreign patients are least likely to know exists — and the one that, for a specific patient anatomy, produces the most disproportionate satisfaction-to-downtime ratio in the entire Korean cosmetic surgery menu. There is no double-eyelid line being created. There is no skin being cut away. There is no week of bruising and dark glasses. There is just a small fat reduction, a few days of mild swelling, and an upper lid that looks lighter and more rested for years afterward.
If you have searched for “Korean blepharoplasty” or “double-eyelid surgery” and felt like neither name describes what you actually want — if your real complaint is that your eyes look tired even when they aren’t — this is likely the procedure that fits. The consultation in Seoul will tell you whether your anatomy supports it. Clinics that have built reputations in this category — including Link Plastic Surgery — will tell you the truth at the consultation rather than upselling a larger surgical plan. That diagnostic honesty, paired with the technique’s surgical specificity, is the reason this procedure has quietly become one of the under-the-radar specialty exports of the Korean cosmetic surgery industry.