Two patients sat in the same consultation chair on the same morning. Both said the exact same sentence: “I look tired even when I am fully rested.” They were close in age, both had a soft puffiness under the eyes, and both had spent months scrolling Korean clinic photos before booking a flight to Seoul. By the end of their consultations, they walked out with two completely different surgical plans. One was scheduled for fat removal. The other was scheduled for fat repositioning. Neither plan was a mistake. The complaint was identical. The anatomy was not.
This is the part of Korean lower eyelid surgery that most foreign patients never see before they arrive. They search “Korean eye bag removal,” they request it by name, and they assume there is one procedure with one good outcome. In reality, Seoul surgeons run two structurally different operations for the same tired-looking under-eye, and the choice between them is the single decision that determines whether your result still looks good at year five or whether you hollow out and look more exhausted than before you started. If you are weighing this surgery, the smartest first move is a careful consultation at Link Plastic Surgery, where the surgeon checks your specific anatomy before naming a procedure. This guide walks through the decision tree they use, so you understand it before you sit down.

Two Operations, One Complaint: Why the Same Tired Eyes Get Different Surgeries
Let me describe the two patients more precisely, because the difference between them is the whole point.
Patient A was in her early forties. Under each eye she had a clear rounded bulge, the kind that catches a shadow in overhead light and reads as a classic eye bag. When she looked up at the ceiling, the bulge stayed roughly the same. There was no deep groove beneath it, no sunken channel running from the inner corner toward the cheek. Her lower lid skin was on the thicker side and still snapped back quickly when gently pulled. For her, the problem was simple in the best sense: she had too much fat pushing forward, and nothing missing underneath it. The fat was the problem, and removing some of it would flatten the bulge cleanly.
Patient B was in her early thirties. She also had a bulge, but it sat on top of something. Below the puffiness ran a distinct tear-trough hollow, a shadowed groove that deepened when she smiled and looked even darker in side lighting. Her under-eye was not just too full in one spot, it was too full and too empty right next to each other, and the contrast between the bulge and the hollow was exactly what made her look perpetually tired. If a surgeon simply removed her fat, the bulge would flatten but the hollow would remain, and the under-eye would go from “puffy and tired” to “sunken and tired.” Worse over time, not better.
This is the trap that brings so many foreign patients back to Seoul a second time. People request “eye bag removal” because that is the phrase the internet taught them, and a less careful clinic obliges. The phrasing assumes the only issue is excess fat. For a large share of patients, especially anyone under forty, the real issue is fat that has migrated and pooled while the cheek and tear-trough region behind it has thinned and descended. Treat that anatomy with pure removal and you accelerate the very hollowing you were trying to fix. The honest framing a good surgeon gives you on the first visit is that the procedure name should come last, after the anatomy is read, not first because you walked in asking for it.
There is also a language problem hiding inside the consultation that makes this worse for international patients. When you say “eye bag,” you usually mean the whole tired appearance, the puffiness and the shadow and the general sense of looking exhausted. When a surgeon says “eye bag,” they mean one specific thing: a pad of fat herniating forward. Those two definitions overlap but they are not the same, and a patient who walks in confident they want the bag gone is often describing a problem the surgeon would not solve by removing the bag at all. A good consultation slows down at exactly this point and separates what you are seeing in the mirror from what is structurally happening under the skin. The clinics that skip this step are the ones that produce regret, because they treat the word you used instead of the anatomy you have.
To understand which page of the decision tree applies to you, it helps to know the second procedure exists at all, which is exactly what most people requesting removal do not. You can see the dedicated overview of the excision approach on the lower eyelid fat removal page, and the rest of this guide explains when it is right and when it quietly sets you up for a revision.
What Removal Actually Does (and Why It Was the Old Standard)
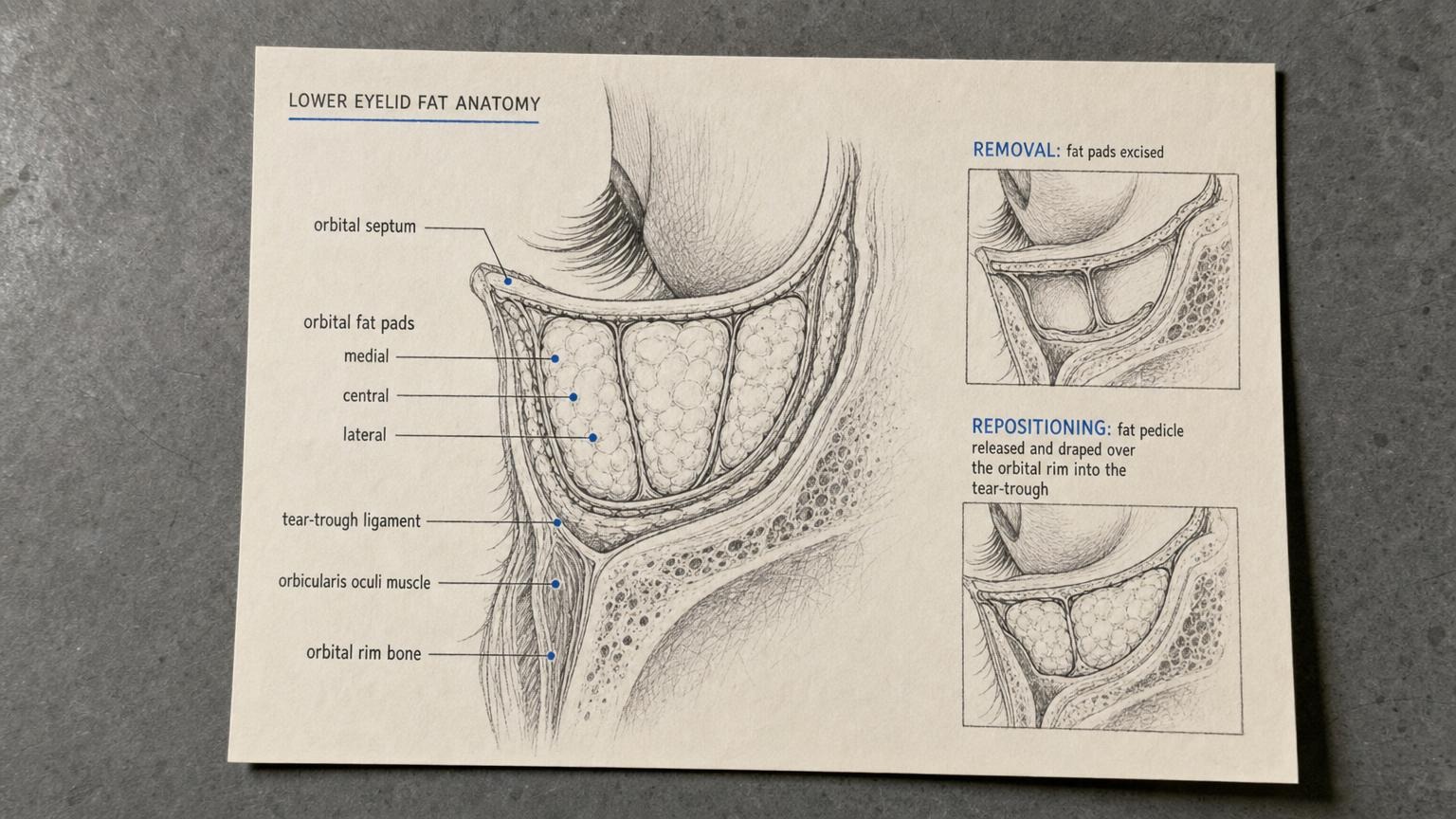
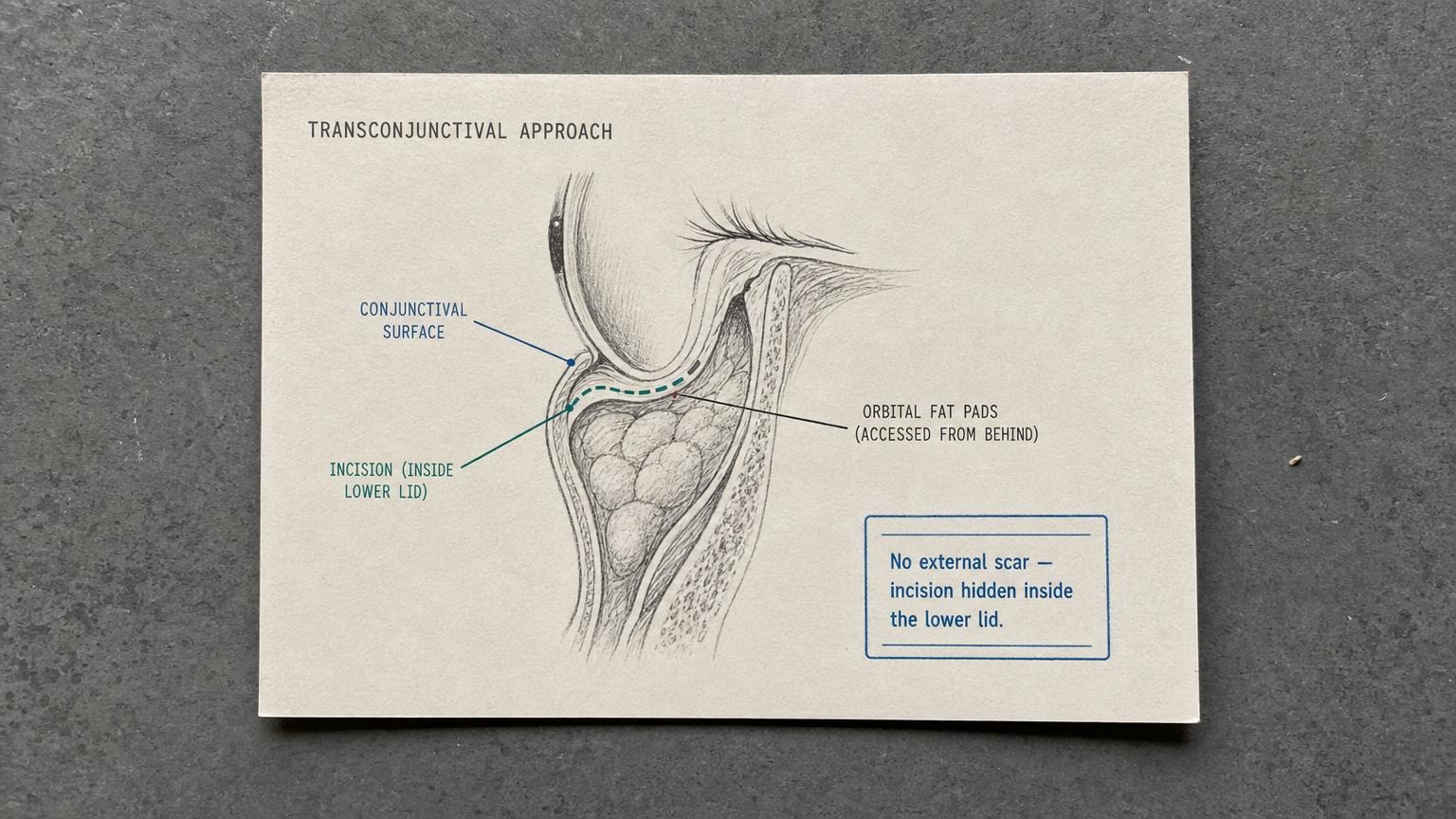
Fat removal under the eye, done the Korean way, is almost always transconjunctival. That word sounds intimidating, but it simply means the incision is made on the inside of the lower lid, on the pink conjunctival surface, rather than on the external skin. There is no visible scar on the outside of the eye. Through that internal opening, the surgeon reaches the three small fat pads that sit behind the lower lid, identifies the ones that are herniating forward and creating the bulge, and trims a measured amount of fat from them.
For the right candidate, this is a genuinely elegant operation. It is fast, often around thirty minutes. It leaves no external scar. Recovery of the visible bruising and swelling is relatively quick. And for someone like Patient A, who has a true excess of fat with no hollow beneath it and skin that still has good elasticity, the result is clean and lasting. The bulge flattens, the under-eye reads as smooth and rested, and there is no downside to having preserved versus removed the fat because there was no hollow that needed filling. This is why removal was the standard approach for decades. When the anatomy matches the procedure, it works beautifully.
The problem is what happens when the anatomy does not match. Take that same removal and perform it on Patient B, the woman with a tear-trough hollow already sitting under the bulge. In the first weeks the result can even look fine, because the swelling masks the groove. Then the swelling resolves, the borrowed volume disappears, and the hollow that was always there is now fully exposed with even less fat in front of it to soften the transition. Over the next two to five years, two things compound the damage. The midface naturally descends with age, deepening the tear-trough groove further. And the eye area, now stripped of fat, has nothing to drape over the rim. The patient who came in looking tired now looks gaunt and hollow, with a dark shadowed trench under each eye that makeup cannot hide.
This single mismatch is the most common reason foreign patients fly back to Seoul for a second surgery. They had removal somewhere, often abroad, often quick and cheap, and two years later they are searching for someone who can put volume back. Restoring volume to an over-removed lower lid is far harder than getting the first operation right, and the menu of fixes is more limited. A surgeon facing an over-removed under-eye is no longer choosing between two clean options. They are working against scar tissue, an established hollow, and a patient who has already lost trust in the process, which is a very different starting point from a first-time consultation.
It is worth being clear about why removal earned its place historically rather than dismissing it. For decades, the prevailing view in many countries was that an eye bag was simply too much fat, and the logical fix for too much of something is to take some away. The thinking was not careless. It matched a real subset of patients, and on those patients it produced good, durable results. What changed is the understanding of the tear trough and the way the midface descends over time. Once surgeons could track their own patients over five and ten years and saw the difference between the eyes they had emptied and the eyes where they had preserved fat, the field shifted. Removal did not become wrong. It became one of two tools, with a much narrower correct use than it once had.
If you are already in the situation of a removal that hollowed you out, the path forward usually runs through a careful revision plan rather than another quick fix, which is its own specialty. The clinic you want is the one that revises this kind of case, not the one that created it, and you can read how that work is approached on the eye revision surgery page.
What Repositioning Does (and Why Korea Made It the Default)
Fat repositioning starts from a different philosophy. The fat is not the enemy. The distribution is. Instead of trimming the herniating fat away, the surgeon releases it from the structures holding it forward, keeps it attached to its own blood supply as a living pedicle, and drapes it downward over the orbital rim into the tear-trough hollow that sits just below.
Recommended for Your Recovery
Products commonly used before and after Korean lower eyelid fat removal vs repositioning decision — same items routinely recommended in the recovery instructions Seoul clinics hand out at discharge.
- Arnica Montana Tablets — begin 3 days before eyelid surgery to reduce periorbital bruising and swelling. Check price on Amazon
- Gel Eye Mask (Cold Compress) — reusable cold pack for the every-two-hour icing schedule on day 1 to day 3. Check price on Amazon
- Silicone Scar Sheets — apply from week 3 onward along the upper lid incision line if your procedure was incisional. Check price on Amazon
- Beauty of Joseon Relief Sun SPF 50+ — lightweight Korean sunscreen to protect the healing scar and prevent post-inflammatory pigmentation. Check price on Amazon
As an Amazon Associate, GlobalBeautySpot earns from qualifying purchases at no extra cost to you.
That one move solves two problems at the same time. The bulge flattens, because the fat is no longer pushing straight forward. And the hollow fills, because the same fat is now redistributed into the groove that was creating the dark shadow. The result is a smooth, continuous transition from the lower lid down onto the cheek, with no sharp step between full and empty. The under-eye reads as one gentle plane instead of a bump sitting above a ditch. Repositioning is not fat removal performed more gently. It is a different operation with a different goal, which is why the outcomes age so differently.
Korea did not adopt repositioning as the default by accident. The Korean aesthetic for the under-eye prioritizes a smooth, youthful, lightly cushioned surface rather than a flat, scooped one, and surgeons watching their own long-term results learned that preserving and relocating fat ages far better than excising it. A repositioned lower lid still has its native fat in the region, so as the face matures it has reserves to draw on instead of an empty hollow that only deepens.
The technical demand of repositioning is the honest reason not every clinic does it well. Releasing the fat without cutting off its blood supply, draping it smoothly over a bony rim, and anchoring it in the right plane so it neither bulges again nor disappears into the cheek is genuinely difficult work, and it shows in the result. A poorly executed repositioning can leave lumps, an uneven contour, or a faint ridge where the fat was secured. This is not an argument against the procedure. It is an argument for choosing a surgeon who does a high volume of these and can show you their own long-term outcomes rather than a marketing gallery. The skill gap between an average lid surgeon and an eye specialist is wider in repositioning than in almost any other facial procedure, precisely because the margin for error is small and the anatomy is unforgiving.
The trade-off is otherwise honest: repositioning is more technically demanding, the operation takes longer, and the early swelling can last a bit longer because more tissue was handled. But for the large group of patients who have any tear-trough hollow at all, the stability over the years is the entire reason it has become the standard recommendation. The detailed overview of the technique and who suits it lives on the under-eye fat repositioning page.

The Decision Tree: How Seoul Surgeons Choose in Five Minutes
When a careful surgeon sits across from you, the choice between removal and repositioning is not a coin flip and it is not a sales decision. It is a short anatomical assessment that an experienced eye specialist runs in about five minutes. Here is the sequence, so you can watch for it.
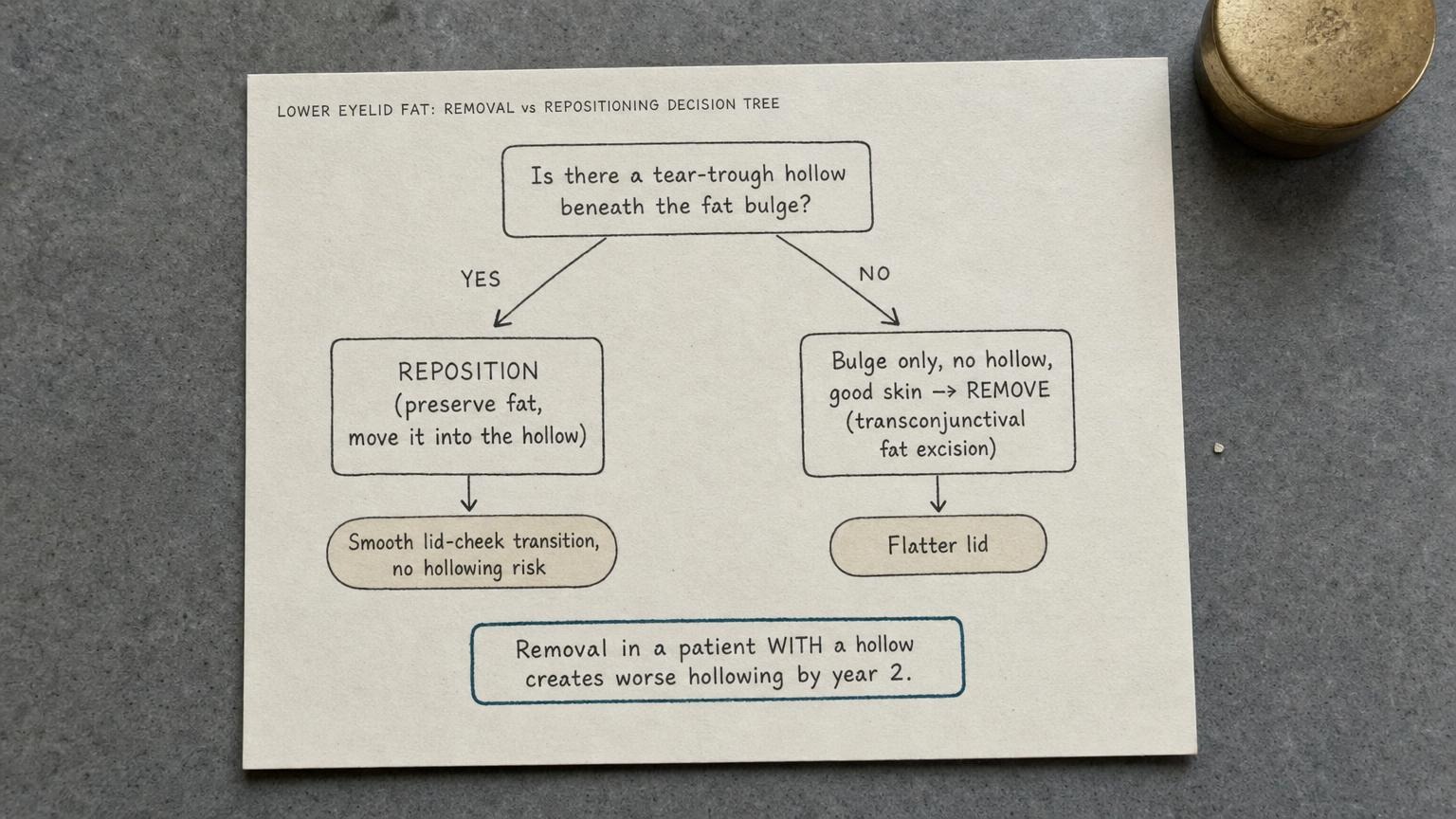
Test one: is there a tear-trough hollow under the bulge? This is the master question. The surgeon has you look straight ahead, then up at the ceiling, then down at the floor, watching how the bulge and the groove behave in changing light. The classic sign is a bulge sitting directly above a shadowed channel that runs from the inner corner toward the cheek. If that hollow is present, repositioning jumps to the front of the line, because removal would expose and deepen it.
Test two: skin quality and elasticity. A gentle pinch of the lower lid skin, watching how fast it springs back, tells the surgeon whether the skin envelope can be left alone or whether loose, crepey skin needs its own attention. Poor elasticity sometimes means the fat work has to be paired with a skin-tightening step, which changes the surgical plan beyond the fat question.
Test three: how much fat, and where. A small bulge sitting over a big hollow is a textbook repositioning case, because there is little excess to remove and plenty of empty space to fill. A large bulge with no hollow underneath is the cleaner removal case, because there is genuine excess and nowhere that needs volume. Many patients fall in between, which is where the hybrid plan in the next section comes in.
Test four: age and midface projection. Younger patients, especially those in their twenties and thirties, almost always reposition, because their problem is far more often malposition and early hollowing than true fat excess. The older the patient and the more genuine the herniation, the more removal or a hybrid enters the conversation.
Test five: negative vector assessment. If your eyeball sits relatively prominent and your cheekbone is comparatively flat, that combination, called a negative vector, changes everything. A negative-vector lower lid is more prone to pulling down and showing white below the iris after aggressive surgery, so the plan has to be more conservative and more often favors gentle repositioning with extra support rather than removal.
The honest rule that falls out of this tree is uncomfortable but worth saying plainly: most foreign patients who walk in asking for “removal” are actually repositioning candidates. They have a hollow they have not been taught to notice, and the bulge is only half their problem. A clinic that books you for removal without ever checking for a tear-trough hollow is, frankly, the clinic you will be revising away from in two years. If you want to understand how the diagnostic side of this works before your consultation, the broader breakdown of under-eye types lives on the eye surgery hub page, which is a useful primer on telling a hollow apart from a bag in the first place.
Cost, Recovery, and the Hybrid Option
Once the right procedure is identified, the practical questions follow: what does it cost, what does recovery look like, and what happens when your two eyes do not need the same thing.
Pricing in Korea is meaningfully lower than in the West for the same level of surgical skill, and the gap between removal and repositioning reflects the added complexity of preserving and relocating fat rather than simply trimming it.
| Procedure / Region | Approximate Price | Notes |
|---|---|---|
| Lower eyelid fat removal (Korea) | KRW 1.5M to 2.5M | Transconjunctival, no external scar |
| Fat repositioning (Korea) | KRW 2.5M to 4M | Higher skill, longer surgery, ages better |
| Comparable surgery (USA) | USD 4,000 to 8,000+ | Often quoted as lower blepharoplasty |
| Comparable surgery (Australia) | AUD 6,000 to 11,000+ | Varies widely by surgeon and city |
Recovery for the transconjunctival approach is gentler than people expect, largely because there is no external skin incision to heal. The visible bruising and swelling typically settle enough to return to normal social life within one to two weeks, with concealer covering most of what remains. The deeper tissue settling, where the final smoothness reveals itself, takes two to three months, and repositioning sits at the longer end of that range because more tissue was moved. You should not judge your final result at week two. The under-eye is one of the last areas to fully settle, and early lumpiness or unevenness in a repositioning case usually smooths out as the relocated fat integrates.
Then there is the hybrid option, which is where surgical judgment really separates the good clinics from the rest. Real faces are rarely symmetrical, and the two eyes often do not need the identical operation. A common pattern is a patient who needs fat repositioned medially, toward the inner corner where the tear-trough hollow is deepest, while a small amount of fat is trimmed laterally, toward the outer corner where a genuine bulge persists with no hollow beneath it. The best surgeons mix techniques within the same surgery, and sometimes differently between the left and right eye, because they are treating the anatomy in front of them rather than applying one label to both sides. For patients with significant overall volume loss across the whole midface, the plan sometimes extends to adding volume directly, and you can read how structural fat grafting fits alongside lid surgery on the facial fat grafting page.
Before you commit anywhere, run this five-question verification at your consultation. One, did the surgeon actually check for a tear-trough hollow, with the look-up and look-down test, before naming a procedure? Two, will they reposition or remove, and can they explain why in plain anatomical terms specific to your face? Three, is it transconjunctival, so there is no external scar? Four, what is the realistic year-five outlook for your particular anatomy, not a generic before-and-after? Five, who handles your remote follow-up after you fly home, and how? A clinic that answers all five clearly is a clinic that read your anatomy instead of your search history.

Frequently Asked Questions
Will fat removal really hollow me out over time?
Only if you had a tear-trough hollow to begin with and the surgeon removed fat anyway. For a patient with a true fat excess and no hollow, removal stays stable for years. The hollowing problem happens when removal is performed on someone who needed repositioning, because the groove that was always there gets exposed and then deepens as the midface descends with age. This is why the hollow check is the most important part of the consultation. It is not the procedure that hollows you out. It is the wrong procedure for your anatomy.
Can repositioning be done after a botched removal?
It is much harder than getting it right the first time, and the options are more limited. Once fat has been removed it is gone, so a surgeon cannot reposition what is no longer there. Revision usually means adding volume back through structural fat grafting or other techniques rather than relocating existing fat, and the results, while often a real improvement, rarely match the smoothness of a correct first operation. This is precisely why the first surgical decision matters so much and why over-removed patients become revision cases.
How is this different from under-eye filler?
Filler is a temporary, non-surgical way to camouflage a hollow by injecting volume into the tear trough, and it lasts months to a year or two before it needs topping up. It does nothing about a fat bulge, and injected too aggressively under thin lower-lid skin it can puff, migrate, or cast a bluish tint. Surgery addresses the underlying structure permanently by either removing or relocating your own fat. Filler can be a reasonable trial for a pure mild hollow, but it cannot fix a bulge-over-hollow combination the way repositioning does.
Can this be combined with fat grafting?
Yes, and for patients with broader midface volume loss it often should be. Repositioning handles the immediate under-eye transition, while structural fat grafting can restore volume across the cheek and surrounding regions that have thinned with age. Combining them in one surgery gives a more harmonious overall result than treating the lower lid in isolation, and an experienced surgeon will tell you during the consultation whether your face is a single-area case or a fuller-face plan.
Is there really no external scar with the transconjunctival approach?
Correct. The incision is made on the inner, pink surface of the lower lid, so nothing is cut on the outside skin and there is no visible external scar. This is the standard approach for both removal and repositioning in younger patients with reasonable skin quality. The exception is when significant excess skin also needs to be trimmed, which may require a fine external incision just below the lash line, but that is a separate decision the surgeon makes based on your skin, not a default.
Do Asian and Western lower lids need different planning?
To a degree, yes. Asian lower-lid skin and the surrounding soft tissue tend to behave differently from thinner Western lids, and the Korean preference for a smooth, lightly cushioned under-eye shapes how aggressively fat is handled. Korean surgeons are trained heavily on Asian anatomy, but experienced eye specialists routinely plan for both, adjusting the amount of fat moved and the support given to the lid based on the individual face rather than a one-size template.
What is the recovery downtime realistically?
Plan for one to two weeks before you look socially presentable, with bruising and swelling that concealer can largely cover toward the end of that window. There is no external scar to fuss over with the transconjunctival approach. The deeper settling, where the final smooth result emerges, takes two to three months, and repositioning sits at the longer end because more tissue was relocated. Do not panic at early unevenness. It typically resolves as the tissue integrates.
Will the result last?
A correctly chosen procedure on the right anatomy is stable for many years. Repositioning ages particularly well because your own fat is preserved in the region and has reserves to draw on as the face matures. Removal also lasts when it was the right call, meaning there was genuine excess and no hollow. No surgery freezes the aging process entirely, but the right operation means you continue to look rested rather than progressively more tired, which is the opposite of what a mismatched procedure does.
What kind of anesthesia is used?
Lower eyelid fat surgery in Korea is typically performed under local anesthesia combined with light sedation, so you are comfortable and relaxed without the burden of general anesthesia. The transconjunctival approach is well suited to this, and being able to cooperate gently during the procedure can actually help the surgeon assess symmetry. Your specific plan is confirmed during the consultation based on the extent of the surgery and your own comfort.
How long should I stay in Seoul for this?
A practical stay is around seven to ten days. That allows time for the consultation and surgery, a few days of initial swelling to come down, and at least one in-person follow-up before you fly home. The visible bruising will not be fully gone by departure, but it will be manageable with concealer. After you return home, reputable clinics arrange remote follow-up so your recovery is monitored, which is one of the five questions worth confirming before you book. To start that conversation and have your anatomy assessed properly, the best first step is to reach out through Link Plastic Surgery’s official website and request a detailed consultation rather than naming a procedure in advance.